

[Endoscopic negative pressure treatment : From management of complications to pre-emptive active reflux drainage in abdominothoracic esophageal resection-A new safety concept for esophageal surgery]
- PMID: 37882839
- PMCID: PMC10689535
- DOI: 10.1007/s00104-023-01970-2
[Endoscopic negative pressure treatment : From management of complications to pre-emptive active reflux drainage in abdominothoracic esophageal resection-A new safety concept for esophageal surgery]
Abstract
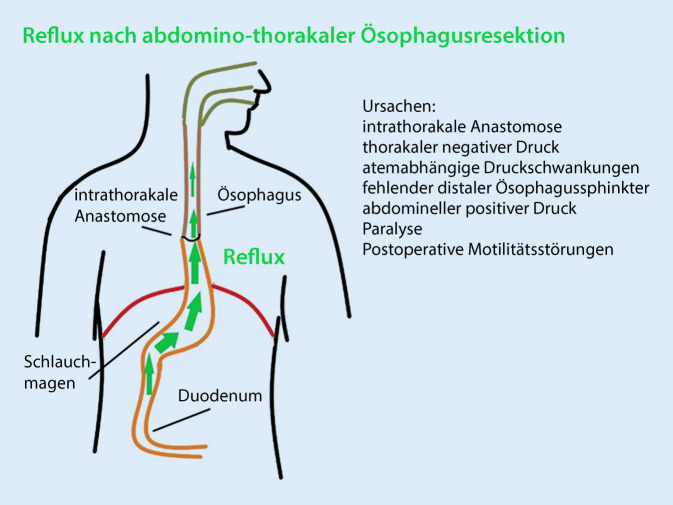
Introduction: Early postoperative reflux (PR) can compromise anastomotic healing after Ivor Lewis esophagectomy (ILE) and poses a risk for aspiration. Anastomotic insufficiency is the most threatening surgical complication. We present the protective method of pre-emptive active reflux drainage (PARD) with simultaneous enteral feeding. We report our experience with this new safety concept in esophageal surgery in a cohort of 43 patients.
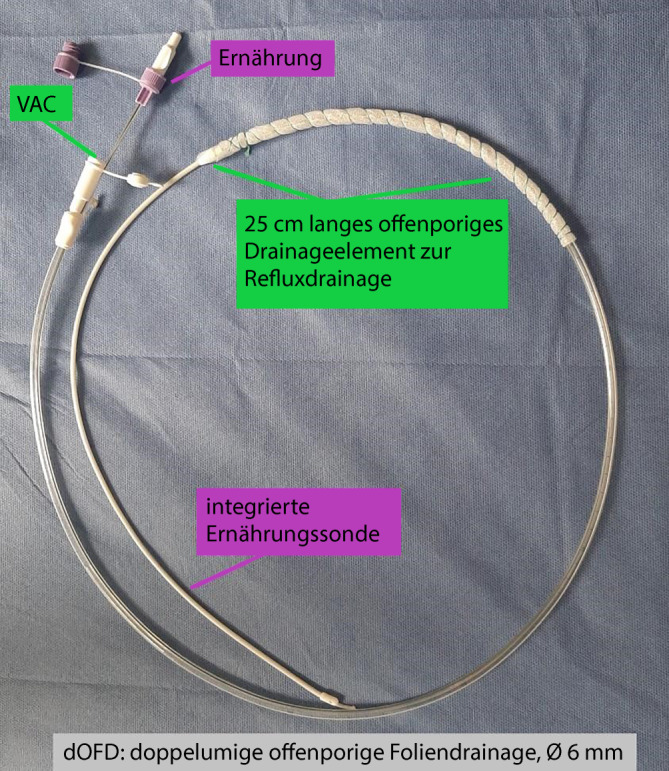
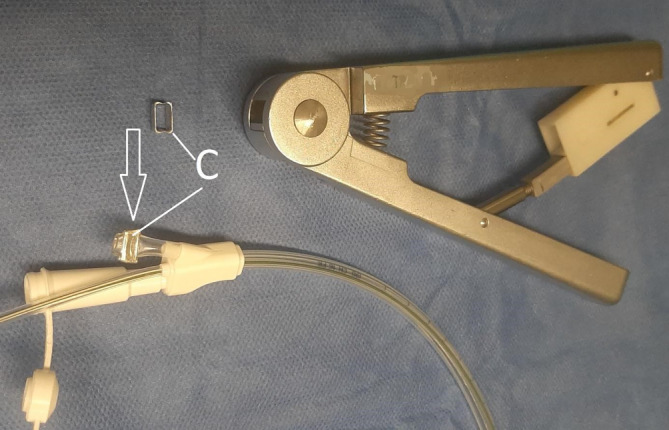
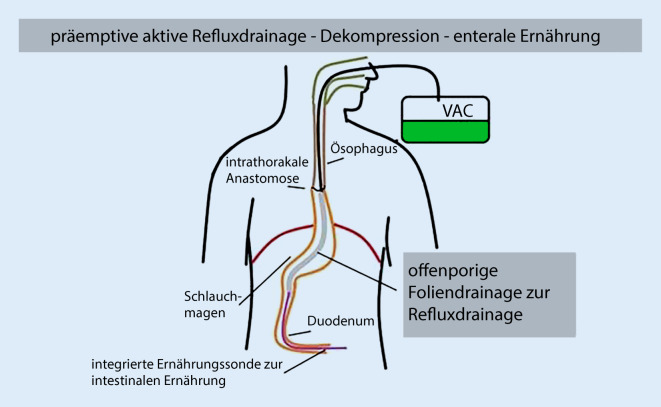
Materials and methods: For PARD we use a double lumen open porous film drainage (dOFD). To create the dOFD, the gastric tube of a Trelumina probe (Freka®Trelumina, Fresenius) is coated with a double-layered open-pore drainage film (Suprasorb®CNP drainage film, Lohmann & Rauscher) over a length of 25 cm. The dOFD is endoscopically inserted into the tubular stomach intraoperatively after completion of the anastomosis. Continuous negative pressure is applied with an electronic pump (-125 mm Hg). The PR is continuously aspirated completely and the stomach and anastomotic region are decompressed. At the same time, nutrition is delivered via an integrated intestinal tube. Depending on the results of the endoscopic control after 5 days, PARD is either continued or terminated.
Results: During the observation period (2017-2023), PARD was used in all patients (n = 43) with ILE. The healing rate under PARD was 100% and healing was observed in all anastomoses. No additional endoscopic procedures or surgical revisions of the anastomoses were required. The median duration of PARD was 8 days (range 4-21). We observed problems in the healing of the anastomosis in 20 of 43 patients (47%) for whom we defined endoscopic criteria for at-risk anastomosis.
Conclusions: Our results suggest that PARD has a strong protective effect on anastomotic healing and may reduce the risk of anastomotic insufficiency. The integrated feeding tube of the dOFD allows early postoperative enteral feeding while simultaneously applying negative pressure. PARD appears to prevent the negative consequences of impaired anastomotic healing.
Zusammenfassung: EINLEITUNG: Der früh postoperative Reflux (PR) kann die Anastomosenheilung nach Ivor-Lewis-Ösophagektomie (ILE) beeinträchtigen und stellt ein Risiko für Aspirationen dar. Die Anastomoseninsuffizienz ist die bedrohlichste chirurgische Komplikation.Wir stellen die protektive Methode der pre-emptiven aktiven Refluxdrainage (PARD) mit gleichzeitiger enteraler Ernährung vor. Wir berichten über unsere Erfahrungen mit dem neuen Sicherheitskonzept für die Ösophaguschirurgie an einem Patientenkollektiv von 43 Patienten.
Materialien und methoden: Zur PARD nutzen wir eine doppellumige offenporige Foliendrainage (dOFD). Zur Herstellung der dOFD wird der gastrale Schenkel einer Trelumina Sonde (Freka®Trelumina, Fresenius) über eine Länge von 25 cm mit einer doppellagigen offenporigen Drainagefolie (Suprasorb®CNP Drainagefolie, Lohmann & Rauscher) beschichtet. Die dOFD wird nach Fertigstellung der Anastomose intraoperativ endoskopisch im Schlauchmagen eingeführt. Es wird ein kontinuierlicher Unterdruck mit einer elektronischen Pumpe angelegt (−125 mm Hg). Der PR wird permanent komplett abgesaugt, der Magen und die Anastomosenregion dekomprimiert. Gleichzeitig wird über eine integrierte Intestinalsonde ernährt. Je nach den Ergebnissen der endoskopischen Kontrolle nach 5 Tagen wird PARD entweder fortgesetzt oder beendet.
Ergebnisse: Im Beobachtungszeitraum (2017–2023) wurde PARD bei allen Patienten (n = 43) mit ILE eingesetzt. Die Heilungsrate unter PARD betrug 100 %, bei allen Anastomosen wurde eine Abheilung beobachtet. Es wurden keine zusätzlichen endoskopischen Eingriffe oder chirurgische Revisionen an den Anastomosen erforderlich. Die mediane Dauer der PARD betrug 8 Tage (Spanne 4–21). Bei 20 von 43 Patienten (47 %) sahen wir Probleme in der Anastomosenheilung, für die wir endoskopische Kriterien der Risikoanastomose definierten.
Schlussfolgerung: Unsere Ergebnisse legen nahe, dass PARD einen starken protektiven Effekt auf die Anastomosenheilung hat und das Risiko der Anastomoseninsuffizienz reduzieren kann. Die integrierte Ernährungssonde der dOFD ermöglicht simultan zur Unterdruckausübung die frühpostoperative enterale Ernährung. PARD scheint die negativen Folgen einer gestörten Anastomosenheilung zu verhindern.
Keywords: Anastomosis insufficiency; At-risk anastomosis; Intraluminal endoscopic vacuum therapy; Prevention; Prophylaxis.
© 2023. The Author(s).



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials