

Vosoritide Therapy in Children with Achondroplasia: Early Experience and Practical Considerations for Clinical Practice
- PMID: 37882884
- PMCID: PMC10796712
- DOI: 10.1007/s12325-023-02705-9
Vosoritide Therapy in Children with Achondroplasia: Early Experience and Practical Considerations for Clinical Practice
Abstract
Introduction: Vosoritide is the first precision medical therapy approved to increase growth velocity in children with achondroplasia. Sharing early prescribing experiences across different regions could provide a framework for developing practical guidance for the real-world use of vosoritide.
Methods: Two meetings were held to gather insight and early experience from experts in Europe, the Middle East, and the USA. The group comprised geneticists, pediatric endocrinologists, pediatricians, and orthopedic surgeons. Current practices and considerations for vosoritide were discussed, including administration practicalities, assessments, and how to manage expectations.
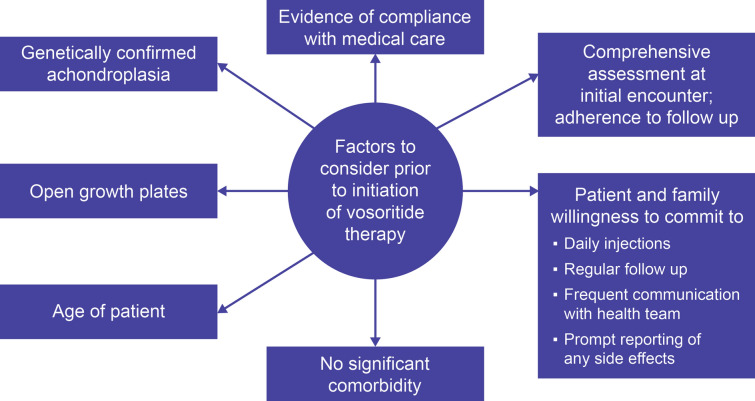
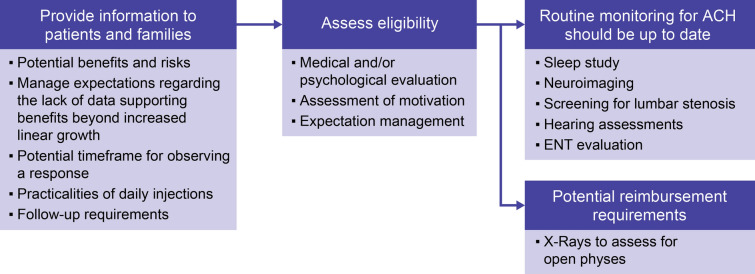
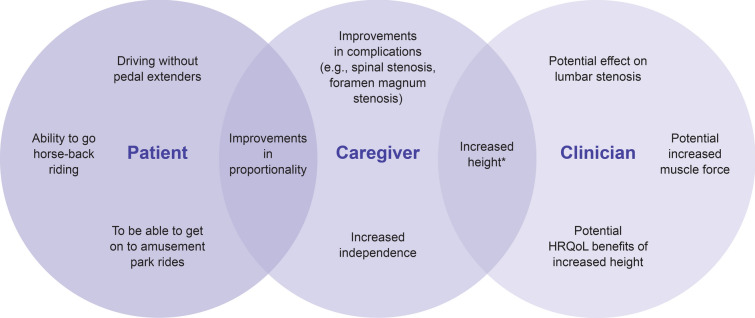
Results: A crucial step in the management of achondroplasia is to determine if adequate multidisciplinary support is in place. Training for families is essential, including practical information on administration of vosoritide, and how to recognize and manage injection-site reactions. Advocated techniques include establishing a routine, empowering patients by allowing them to choose injection sites, and managing pain. Patients may discontinue vosoritide if they cannot tolerate daily injections or are invited to participate in a clinical trial. Clinicians in Europe and the Middle East emphasized the importance of assessing adherence to daily injections, as non-adherence may impact response and reimbursement. Protocols for monitoring patients receiving vosoritide may be influenced by regional differences in reimbursement and healthcare systems. Core assessments may include pubertal staging, anthropometry, radiography to confirm open physes, the review of adverse events, and discussion of concomitant or new medications-but timing of these assessments may also differ regionally and vary across institutions. Patients and families should be informed that response to vosoritide can vary in both magnitude and timing. Keeping families informed regarding vosoritide clinical trial data is encouraged.
Conclusion: The early real-world experience with vosoritide is generally positive. Sharing these insights is important to increase understanding of the practicalities of treatment with vosoritide in the clinical setting.
Keywords: Achondroplasia; Assessments; Clinical practice; Early experience; Guidance; Management; Monitoring; Practicalities; Vosoritide.
© 2023. The Author(s).
Conflict of interest statement
In addition to the individual conflict of interest outlined below, all authors participated in the expert group meetings, sponsored and organized by BioMarin Pharmaceutical Inc, on which this manuscript is based. Oliver Semler: has received grants or contracts from Kyowa Kirin, payment or honoraria for lectures/presentations from BioMarin and Kyowa Kirin, and support for attending meetings and/or travel from Pfizer. Valérie Cormier-Daire: has received payment or honoraria for lectures/presentations from BioMarin and Ipsen, and participated in Advisory Board meetings for BioMarin, QED-Propel and Mereo. Ekkehart Lausch: has received grants or contracts from DFG (SFB1453), H2020, consulting fees, support for attending meetings and/or travel, and has participated in Advisory Board meetings for BioMarin. Michael B. Bober: has received grants or contracts from BioMarin, Ascendis, QED and Pfizer (all Institutional), consulting fees from BioMarin and Tyra (Institutional), Ascendis and Bridge Bio, payment or honoraria for lectures/presentations from NovoNordisk and Tyra, has participated in Advisory Board meetings for BioMarin, and has a leadership role for the Skeletal Dysplasia Management Consortium. Ricki Carroll: has received grants or contracts from BioMarin, QED, Ascendis and Pfizer (all Institutional), and consulting fees from Guidepoint. Sérgio B. Sousa: has received payment or honoraria for lectures/presentations, support for attending meetings and/or travel, and has participated in Advisory Board meetings for BioMarin, and has a leadership role for the European Achondroplasia Forum and ERN-BOND. David Deyle: has received grants or contracts from Castle Creek. Maha Faden: has received support for attending meetings and/or travel, and has participated in Advisory Board meetings for BioMarin. Gabriele Hartmann: has received consulting fees, support for attending meetings and/or travel, and has participated in Advisory Board meetings for BioMarin. Aaron J. Huser: has received payment or honoraria for speaker bureau, has participated in Advisory Board meetings for BioMarin, and holds a leadership role for the MHE Research Foundation. Janet M. Legare: has received grants or contracts for clinical trials from Ascendis Pharma and Bridge Bio, and for a natural history study from BioMarin, and payment or honoraria for lectures/presentations from BioMarin. Klaus Mohnike: has received grants or contracts for clinical trials, payment or honoraria for lectures/presentations, support for attending meetings and/or travel and has participated in Advisory Board meetings for BioMarin. Tilman R. Rohrer: has received grants or contracts, consulting fees, payment or honoraria for lectures/presentations and support for attending meetings and/or travel from BioMarin and NovoNordisk. Frank Rutsch: has received grants or contracts (Institutional), consulting fees, payment or honoraria for lectures/presentations, support for attending meetings and/or travel, and has participated in Advisory Board meetings for BioMarin. Pamela Smith: has received payment or honoraria for lectures/presentations, and support for attending meetings and/or travel from BioMarin. Andre M. Travessa: has received consulting fees, support for attending meetings and/or travel, and participated in Advisory Board meetings. Angela Verardo: Has received payment or honoraria for speaker bureau from BioMarin. Klane K. White: Has received grants or contracts from BioMarin, Ascendis, Ultragenyx and Pfizer, royalties or licenses for UptoDate.com, payment or honoraria for lectures/presentations from BioMarin and has a leadership role for Little People of America, National MPS Society, Pediatric Orthopedic Society of North America, Scoliosis Research Society, Camp Korey, and the Skeletal Dysplasia Management Consortium. William R. Wilcox: has received grants or contracts (Institutional), and has participated in Advisory Board meetings for BioMarin. Julie Hoover-Fong: has received grants or contracts for clinical trials from BioMarin, QED and Pfizer, consulting fees from BioMarin, QED, NovoNordisk and Innoskel, payment or honoraria for lectures/presentations from Medscape and BioMarin, has participated in Advisory Board meetings for MCDS—Therapy Clinical Trial (unpaid), BioMarin and QED, and is an unpaid member of the Skeletal Dysplasia Management Consortium and of the Medical Advisory Board of the Little People of America.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
