

Risk Model-Based Lung Cancer Screening and Racial and Ethnic Disparities in the US
- PMID: 37883107
- PMCID: PMC10603577
- DOI: 10.1001/jamaoncol.2023.4447
Risk Model-Based Lung Cancer Screening and Racial and Ethnic Disparities in the US
Abstract
Importance: The revised 2021 US Preventive Services Task Force (USPSTF) guidelines for lung cancer screening have been shown to reduce disparities in screening eligibility and performance between African American and White individuals vs the 2013 guidelines. However, potential disparities across other racial and ethnic groups in the US remain unknown. Risk model-based screening may reduce racial and ethnic disparities and improve screening performance, but neither validation of key risk prediction models nor their screening performance has been examined by race and ethnicity.
Objective: To validate and recalibrate the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial 2012 (PLCOm2012) model-a well-established risk prediction model based on a predominantly White population-across races and ethnicities in the US and evaluate racial and ethnic disparities and screening performance through risk-based screening using PLCOm2012 vs the USPSTF 2021 criteria.
Design, setting, and participants: In a population-based cohort design, the Multiethnic Cohort Study enrolled participants in 1993-1996, followed up through December 31, 2018. Data analysis was conducted from April 1, 2022, to May 19. 2023. A total of 105 261 adults with a smoking history were included.
Exposures: The 6-year lung cancer risk was calculated through recalibrated PLCOm2012 (ie, PLCOm2012-Update) and screening eligibility based on a 6-year risk threshold greater than or equal to 1.3%, yielding similar eligibility as the USPSTF 2021 guidelines.
Outcomes: Predictive accuracy, screening eligibility-incidence (E-I) ratio (ie, ratio of the number of eligible to incident cases), and screening performance (sensitivity, specificity, and number needed to screen to detect 1 lung cancer).
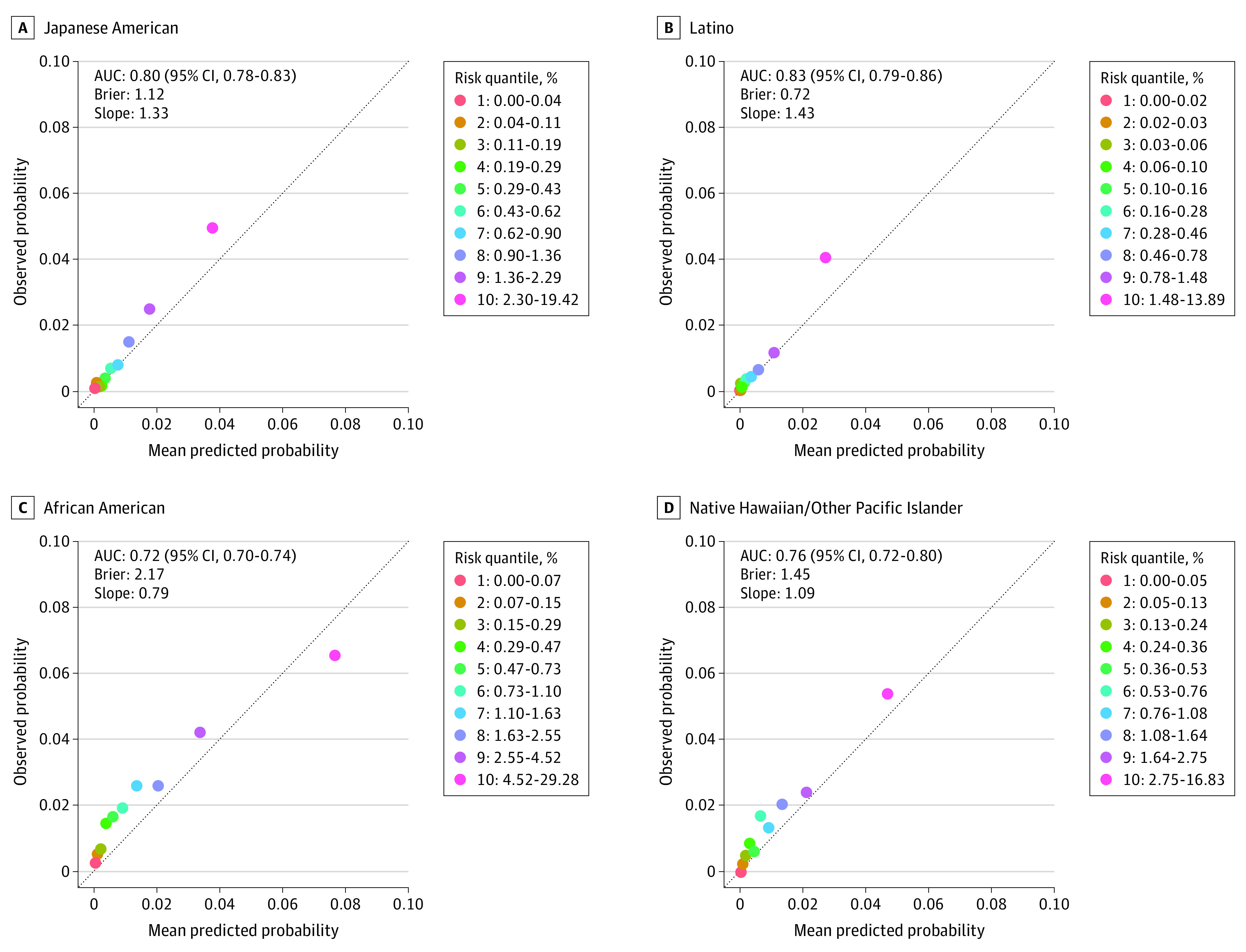
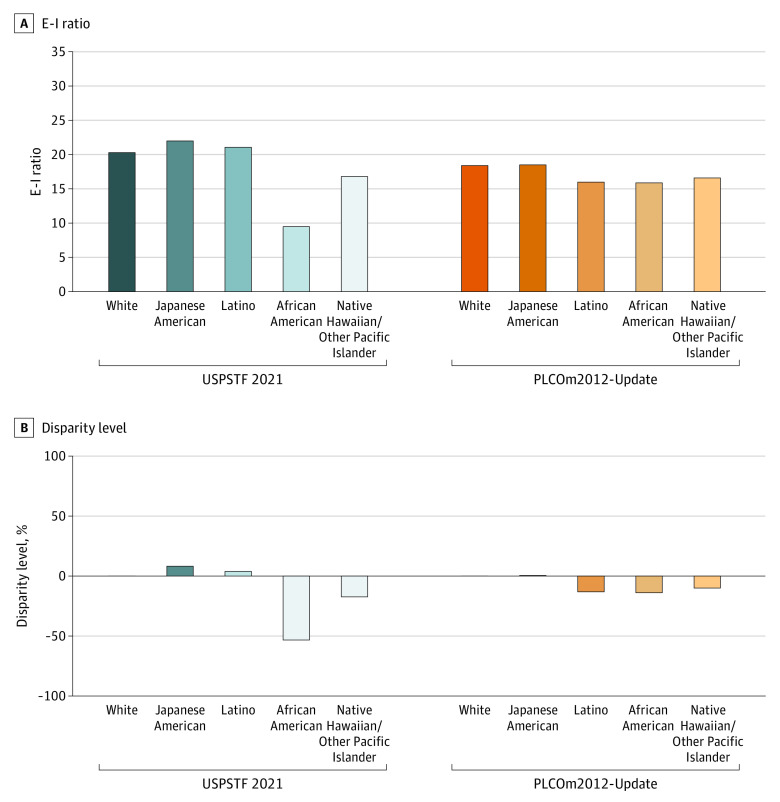
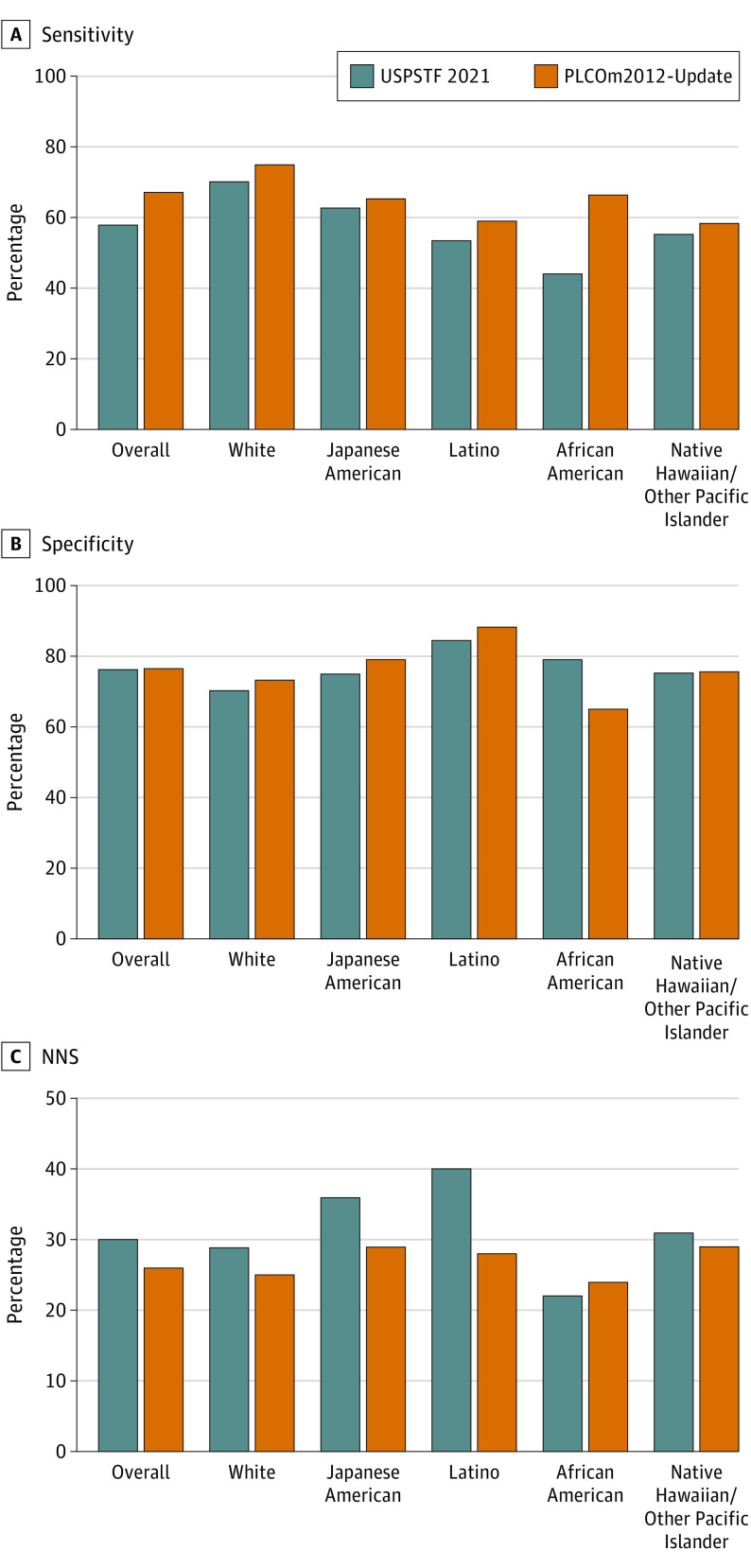
Results: Of 105 261 participants (60 011 [57.0%] men; mean [SD] age, 59.8 [8.7] years), consisting of 19 258 (18.3%) African American, 27 227 (25.9%) Japanese American, 21 383 (20.3%) Latino, 8368 (7.9%) Native Hawaiian/Other Pacific Islander, and 29 025 (27.6%) White individuals, 1464 (1.4%) developed lung cancer within 6 years from enrollment. The PLCOm2012-Update showed good predictive accuracy across races and ethnicities (area under the curve, 0.72-0.82). The USPSTF 2021 criteria yielded a large disparity among African American individuals, whose E-I ratio was 53% lower vs White individuals (E-I ratio: 9.5 vs 20.3; P < .001). Under the risk-based screening (PLCOm2012-Update 6-year risk ≥1.3%), the disparity between African American and White individuals was substantially reduced (E-I ratio: 15.9 vs 18.4; P < .001), with minimal disparities observed in persons of other minoritized groups, including Japanese American, Latino, and Native Hawaiian/Other Pacific Islander. Risk-based screening yielded superior overall and race and ethnicity-specific performance to the USPSTF 2021 criteria, with higher overall sensitivity (67.2% vs 57.7%) and lower number needed to screen (26 vs 30) at similar specificity (76.6%).
Conclusions: The findings of this cohort study suggest that risk-based lung cancer screening can reduce racial and ethnic disparities and improve screening performance across races and ethnicities vs the USPSTF 2021 criteria.
Conflict of interest statement
Figures
Comment in
-
Improving Eligibility Criteria for Lung Cancer Screening-Promises, Challenges, and Unmet Needs.JAMA Oncol. 2023 Dec 1;9(12):1649-1650. doi: 10.1001/jamaoncol.2023.4410. JAMA Oncol. 2023. PMID: 37883100 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
