

Prevalence of Cochlear-Facial and Other Non-Superior Semicircular Canal Third Window Dehiscence on High-Resolution Temporal Bone CT
- PMID: 37884302
- PMCID: PMC10631539
- DOI: 10.3174/ajnr.A8032
Prevalence of Cochlear-Facial and Other Non-Superior Semicircular Canal Third Window Dehiscence on High-Resolution Temporal Bone CT
Abstract
Background and purpose: The radiologic prevalence of superior semicircular canal dehiscence in the asymptomatic population has been widely studied, but less is known about the rates of other forms of third window dehiscence. Per the existing literature, the radiologic prevalence of cochlear-facial nerve dehiscence, for example, exceeds that seen in histologic studies, suggesting that conventional CT is unreliable for cochlear-facial dehiscence. These studies relied on nonisometric CT acquisitions, however, and underused multiplanar reformatting techniques, leading to false-positive findings. Our purpose was to determine the rate of cochlear-facial dehiscence and other non-superior semicircular canal third window dehiscences on optimized CT in asymptomatic patients.
Materials and methods: Sixty-four-channel temporal bone CT scans from 602 patients in emergency departments were assessed for cochlear-facial and other non-superior semicircular canal third window dehiscences by using high-resolution, multiplanar oblique reformats. Confidence intervals for dehiscence prevalence were calculated using the Newcombe 95% interval confidence method.
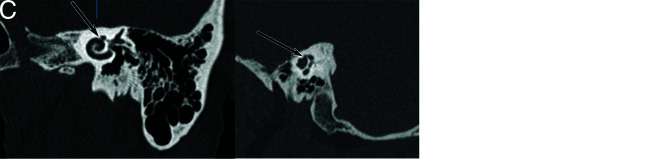
Results: Of 602 patients, 500 were asymptomatic, while 102 had an imaging indication consistent with possible third window syndrome (symptomatic). Eight asymptomatic patients (1.6%) had cochlear-facial dehiscence, while 43 (8.4%) had jugular bulb-vestibular aqueduct dehiscence. There was no statistically significant difference between the prevalence of cochlear-facial dehiscence or jugular bulb-vestibular aqueduct dehiscence in asymptomatic patients compared with symptomatic patients. Cochlear-carotid canal, cochlear-internal auditory canal, and cochlear-petrosal sinus dehiscences were not observed.
Conclusions: Sixty-four-channel CT with multioblique reformatting is sensitive and specific for identifying cochlear-facial dehiscence, with rates similar to those in postmortem series. Jugular bulb-vestibular aqueduct dehiscence is a common incidental finding and is unlikely to produce third window physiology. Other non-superior semicircular canal third window dehiscences are rare in asymptomatic patients.
© 2023 by American Journal of Neuroradiology.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources