

Molecular mechanisms in colitis-associated colorectal cancer
- PMID: 37884500
- PMCID: PMC10603140
- DOI: 10.1038/s41389-023-00492-0
Molecular mechanisms in colitis-associated colorectal cancer
Abstract
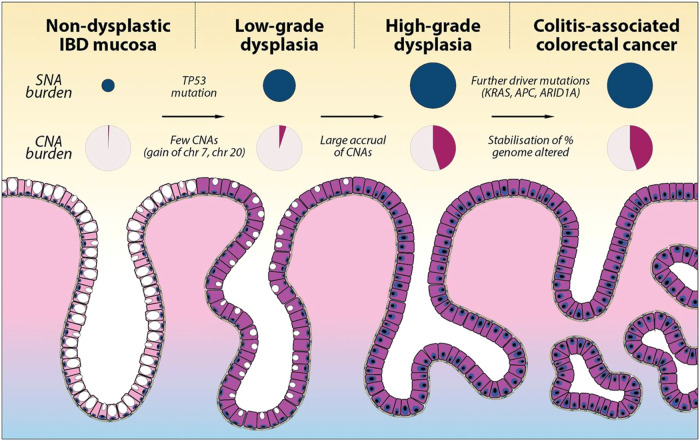
Sustained chronic inflammation of the large intestine leads to tissue damage and repair, which is associated with an increased incidence of colitis-associated colorectal cancer (CAC). The genetic makeup of CAC is somewhat similar to sporadic colorectal carcinoma (sCRC), but there are differences in the sequence and timing of alterations in the carcinogenesis process. Several models have been developed to explain the development of CAC, particularly the "field cancerization" model, which proposes that chronic inflammation accelerates mutagenesis and selects for the clonal expansion of phenotypically normal, pro-tumorigenic cells. In contrast, the "Big Bang" model posits that tumorigenic clones with multiple driver gene mutations emerge spontaneously. The details of CAC tumorigenesis-and how they differ from sCRC-are not yet fully understood. In this Review, we discuss recent genetic, epigenetic, and environmental findings related to CAC pathogenesis in the past five years, with a focus on unbiased, high-resolution genetic profiling of non-dysplastic field cancerization in the context of inflammatory bowel disease (IBD).
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Beaugerie L, Itzkowitz SH. Cancers Complicating Inflammatory Bowel Disease. N Engl J Med. 2015;373:195. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
