Tamoxifen or aromatase inhibitors with ovarian function suppression in pre-menopausal stage I-III lobular breast cancer
- PMID: 37884561
- PMCID: PMC10603127
- DOI: 10.1038/s41523-023-00594-3
Tamoxifen or aromatase inhibitors with ovarian function suppression in pre-menopausal stage I-III lobular breast cancer
Abstract
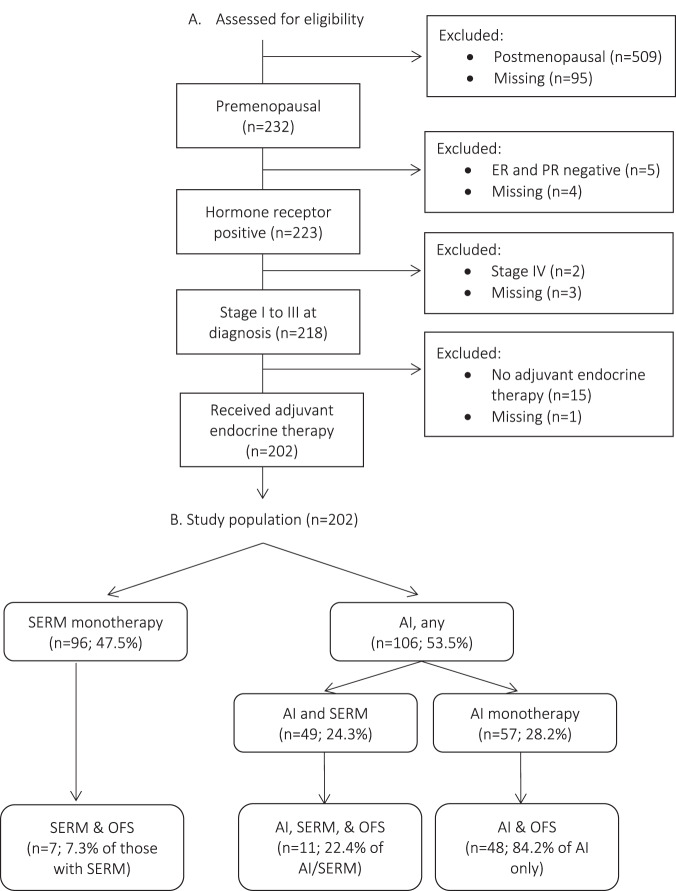
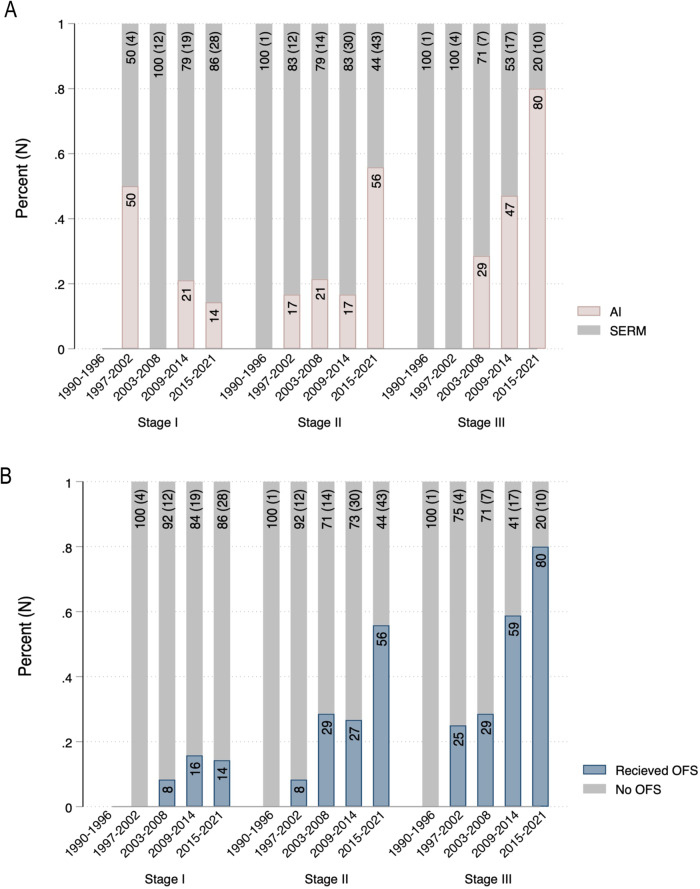
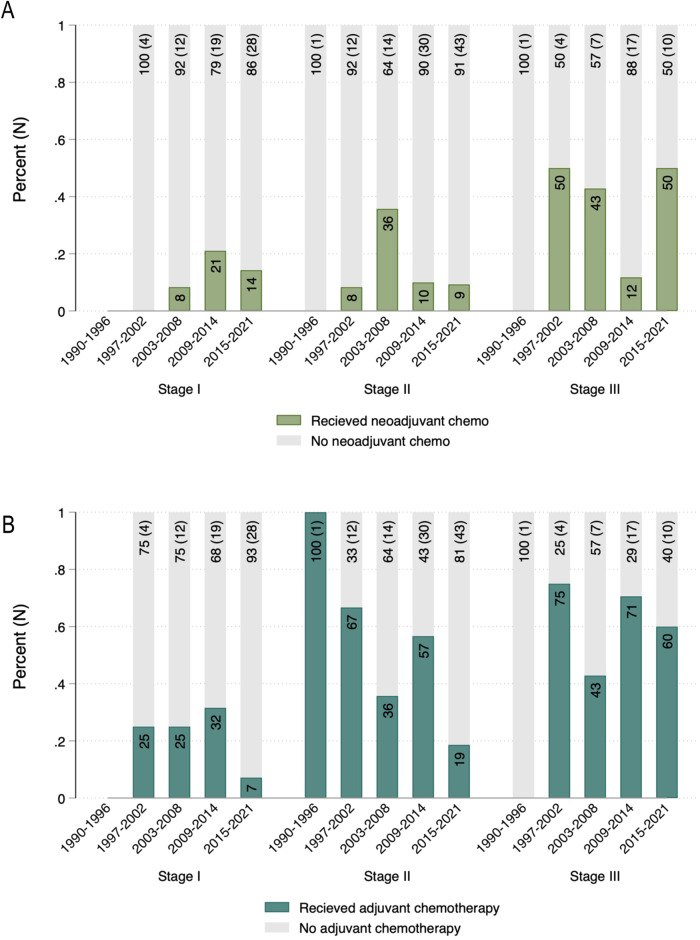
While adjuvant treatment with the selective-estrogen receptor modulator (SERM) tamoxifen has been the standard of care for pre-menopausal patients with hormone receptor (HR) positive breast cancer, recent trials showed a benefit of aromatase inhibitors (AI) and ovarian function suppression (OFS) for some patients. The approach to endocrine therapy has not been well studied in pre-menopausal patients with invasive lobular carcinoma (ILC). We identified 202 pre-menopausal patients with HR positive stage I-III ILC in an institutional database. We investigated factors associated with endocrine therapy type and determined changes in systemic therapy from 1990-2021. We evaluated associations between endocrine therapy type and disease-free survival (DFS) with a multivariate Cox proportional hazards model. Of 202 patients, most (69.3%) were prescribed a SERM (99.3% tamoxifen). Those who received an AI had significantly higher stage disease. Over time, use of OFS and AI increased significantly in stage II or III cases (from 0% in 1990 to 56% after 2015 for stage II; from 0% to 80% after 2015 for stage III). Concurrently, adjuvant chemotherapy use significantly decreased in stage II cases (from 67% to 19%). In an exploratory multivariable model, longer duration of AI compared to tamoxifen was associated with significantly improved DFS (HR 0.31; 95% CI 0.11-0.86; p = 0.025). While most pre-menopausal patients received adjuvant tamoxifen, the use of OFS and AIs increased significantly over time. The association between AI use and improved DFS may be consistent with prior randomized trials and warrants further investigation into predictive factors to guide treatment selection.
© 2023. The Author(s).
Conflict of interest statement
A. Jo Chien receives research funding from Merck, Puma, Amgen, and Seattle Genetics. Michelle E. Melisko reports research funding from Astra Zeneca, Novartis, KCRN Research, Puma, and Seattle Genetics. Hope S. Rugo receives research support for clinical trials through UCSF, Pfizer, Merck, Novartis, Lilly, Roche, Daiichi, Seattle Genetics, Macrogenics, Sermonix, Boehringer Ingelheim, Astra Zeneca, Astellas, and Gilead and honoraria from Puma, Samsung, Mylan, Chugai, Blueprint, and NAPO. All other authors have no competing financial or non-financial interests to disclose. R. Mukhtar is supported by the National Cancer Institute Award K08CA256047.
Figures