

Bladder cancer
- PMID: 37884563
- PMCID: PMC11218610
- DOI: 10.1038/s41572-023-00468-9
Bladder cancer
Abstract
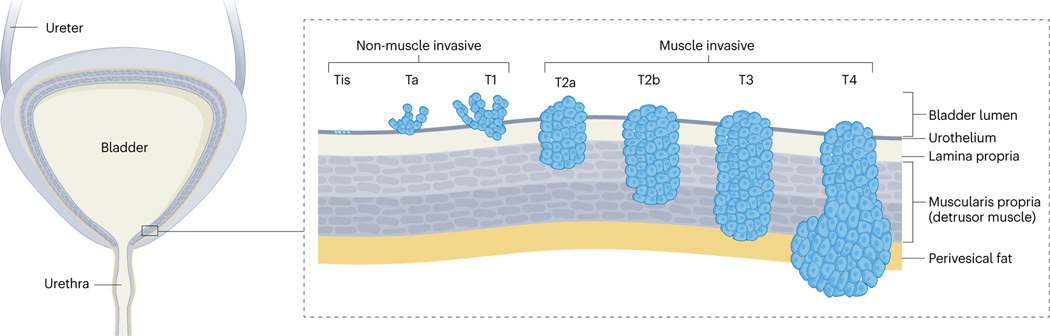
Bladder cancer is a global health issue with sex differences in incidence and prognosis. Bladder cancer has distinct molecular subtypes with multiple pathogenic pathways depending on whether the disease is non-muscle invasive or muscle invasive. The mutational burden is higher in muscle-invasive than in non-muscle-invasive disease. Commonly mutated genes include TERT, FGFR3, TP53, PIK3CA, STAG2 and genes involved in chromatin modification. Subtyping of both forms of bladder cancer is likely to change considerably with the advent of single-cell analysis methods. Early detection signifies a better disease prognosis; thus, minimally invasive diagnostic options are needed to improve patient outcomes. Urine-based tests are available for disease diagnosis and surveillance, and analysis of blood-based cell-free DNA is a promising tool for the detection of minimal residual disease and metastatic relapse. Transurethral resection is the cornerstone treatment for non-muscle-invasive bladder cancer and intravesical therapy can further improve oncological outcomes. For muscle-invasive bladder cancer, radical cystectomy with neoadjuvant chemotherapy is the standard of care with evidence supporting trimodality therapy. Immune-checkpoint inhibitors have demonstrated benefit in non-muscle-invasive, muscle-invasive and metastatic bladder cancer. Effective management requires a multidisciplinary approach that considers patient characteristics and molecular disease characteristics.
© 2023. Springer Nature Limited.
Conflict of interest statement
Competing interests
L.D. has sponsored research agreements with Natera, C2i Genomics, AstraZeneca, Photocure and Ferring, has an advisory/consulting role at Ferring, MSD and UroGen, has received speaker honoraria from AstraZeneca, Pfizer and Roche, and is a board member for BioXpedia. D.E.H. is an advisory board member for AstraZeneca. M.D.G. receives or has received research funding from Bristol Myers Squibb, Novartis, Dendreon, AstraZeneca, Merck and Genentech. M.D.G. is or was a consultant for Bristol Myers Squibb, Merck, Genentech, AstraZeneca, Pfizer, EMD Serono, SeaGen, Janssen, Numab, Dragonfly, GlaxoSmithKline, Basilea, UroGen, Rappta Therapeutics, Alligator, Silverback, Fujifilm, Curis, Gilead, Bicycle, Asieris, Abbvie, Analogue Devices and Veracyte. J.A.E. is or was a consultant/advisory board member and receives or has received honoraria from Blue Earth Diagnostics, Boston Scientific, AstraZeneca, Lantheus, IBA, Astellas, Pfizer, Merck, Roivant Pharma, Myovant Sciences, Janssen, Bayer Healthcare, Progenics Pharmaceuticals, Genentech, Gilead, Angiodynamics and UptoDate. The other authors declare no competing interests.
Figures




References
-
- Sung H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249 (2021). - PubMed
-
- Antoni S. et al. Bladder cancer incidence and mortality: a global overview and recent trends. Eur. Urol. 71, 96–108 (2017). - PubMed
-
- IARC. Global Cancer Observatory: Cancer Tomorrow. WHO; https://gco.iarc.fr/tomorrow/en (2023).
-
- Facchini G. et al. Advanced/metastatic bladder cancer: current status and future directions. Eur. Rev. Med. Pharmacol. Sci. 24, 11536–11552 (2020). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
