

Assessment of hybrid population immunity to SARS-CoV-2 following breakthrough infections of distinct SARS-CoV-2 variants by the detection of antibodies to nucleoprotein
- PMID: 37884642
- PMCID: PMC10603038
- DOI: 10.1038/s41598-023-45718-8
Assessment of hybrid population immunity to SARS-CoV-2 following breakthrough infections of distinct SARS-CoV-2 variants by the detection of antibodies to nucleoprotein
Abstract
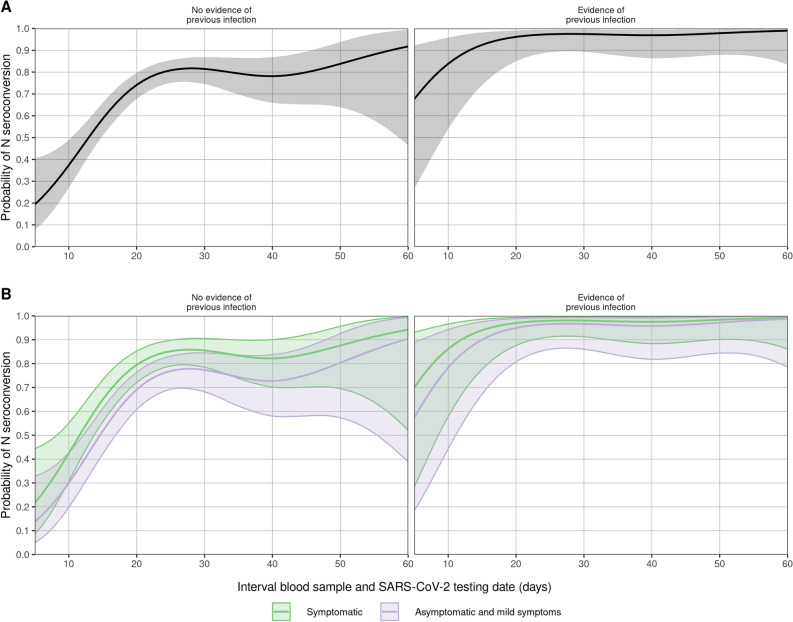
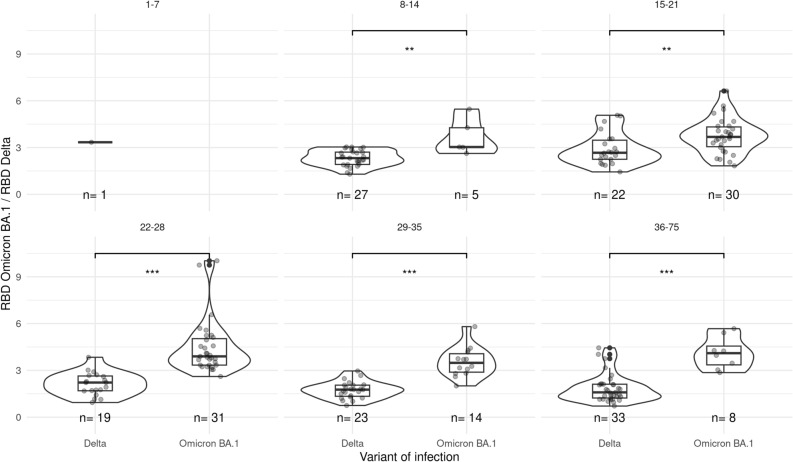
Immunity induced by vaccination and infection, referred to as hybrid immunity, provides better protection against SARS-CoV-2 infections compared to immunity induced by vaccinations alone. To assess the development of hybrid immunity we investigated the induction of Nucleoprotein-specific antibodies in PCR-confirmed infections by Delta or Omicron in vaccinated individuals (n = 520). Eighty-two percent of the participants with a breakthrough infection reached N-seropositivity. N-seropositivity was accompanied by Spike S1 antibody boosting, and independent of vaccination status or virus variant. Following the infection relatively more antibodies to the infecting virus variant were detected. In conclusion, these data show that hybrid immunity through breakthrough infections is hallmarked by Nucleoprotein antibodies and broadening of the Spike antibody repertoire. Exposure to future SARS-CoV-2 variants may therefore continue to maintain and broaden vaccine-induced population immunity.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- WHO Coronavirus (COVID-19) Dashboard, <covid19.who.int> (2022).
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
