

The augmented value of using clinical notes in semi-automated surveillance of deep surgical site infections after colorectal surgery
- PMID: 37884948
- PMCID: PMC10604406
- DOI: 10.1186/s13756-023-01316-x
The augmented value of using clinical notes in semi-automated surveillance of deep surgical site infections after colorectal surgery
Abstract
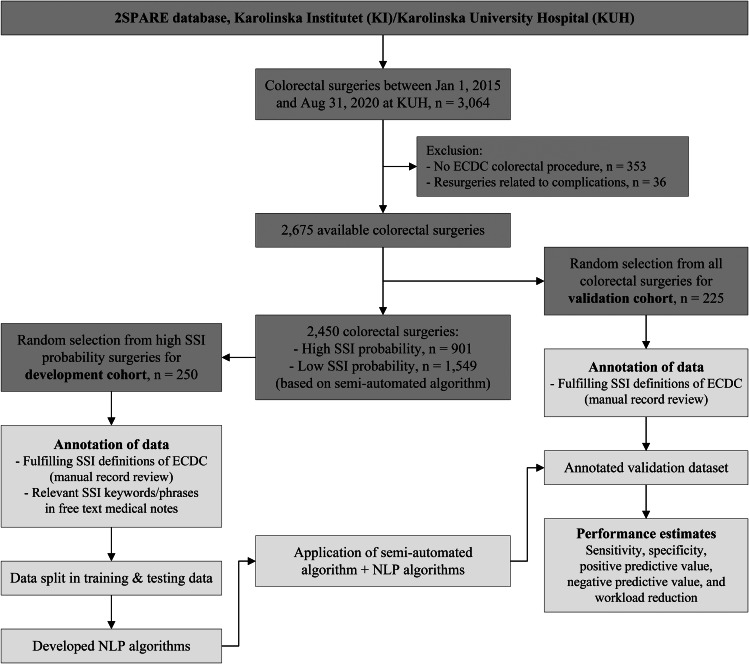
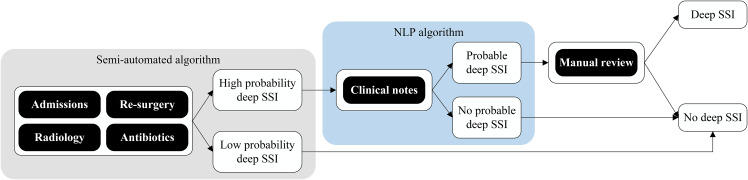
Background: In patients who underwent colorectal surgery, an existing semi-automated surveillance algorithm based on structured data achieves high sensitivity in detecting deep surgical site infections (SSI), however, generates a significant number of false positives. The inclusion of unstructured, clinical narratives to the algorithm may decrease the number of patients requiring manual chart review. The aim of this study was to investigate the performance of this semi-automated surveillance algorithm augmented with a natural language processing (NLP) component to improve positive predictive value (PPV) and thus workload reduction (WR).
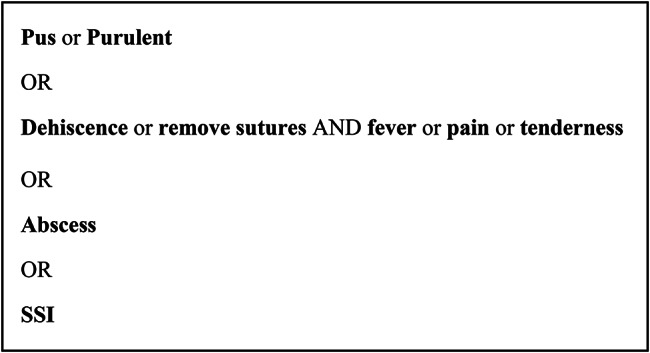
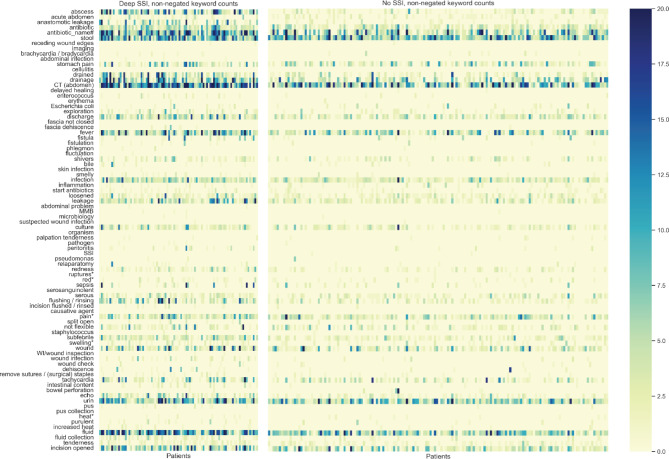
Methods: Retrospective, observational cohort study in patients who underwent colorectal surgery from January 1, 2015, through September 30, 2020. NLP was used to detect keyword counts in clinical notes. Several NLP-algorithms were developed with different count input types and classifiers, and added as component to the original semi-automated algorithm. Traditional manual surveillance was compared with the NLP-augmented surveillance algorithms and sensitivity, specificity, PPV and WR were calculated.
Results: From the NLP-augmented models, the decision tree models with discretized counts or binary counts had the best performance (sensitivity 95.1% (95%CI 83.5-99.4%), WR 60.9%) and improved PPV and WR by only 2.6% and 3.6%, respectively, compared to the original algorithm.
Conclusions: The addition of an NLP component to the existing algorithm had modest effect on WR (decrease of 1.4-12.5%), at the cost of sensitivity. For future implementation it will be a trade-off between optimal case-finding techniques versus practical considerations such as acceptability and availability of resources.
Keywords: Algorithm; Automated surveillance; Colorectal surgery; Healthcare-associated infections; Natural language processing; Surgical site infections.
© 2023. The Author(s).
Conflict of interest statement
PN and SvdW are involved in a company that works on automated surveillance for adverse events. The other authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
