

This is a preprint.
Acute kidney injury following treatment with CD19-specific CAR T-cell therapy in children, adolescent and young adult patients with B-cell acute lymphoblastic leukemia
- PMID: 37886451
- PMCID: PMC10602103
- DOI: 10.21203/rs.3.rs-3396661/v1
Acute kidney injury following treatment with CD19-specific CAR T-cell therapy in children, adolescent and young adult patients with B-cell acute lymphoblastic leukemia
Update in
-
Acute kidney injury following treatment with CD19-specific CAR T-cell therapy in children, adolescent, and young adult patients with B-cell acute lymphoblastic leukemia.Pediatr Nephrol. 2024 Aug;39(8):2495-2503. doi: 10.1007/s00467-024-06331-7. Epub 2024 Mar 20. Pediatr Nephrol. 2024. PMID: 38507119 Free PMC article.
Abstract
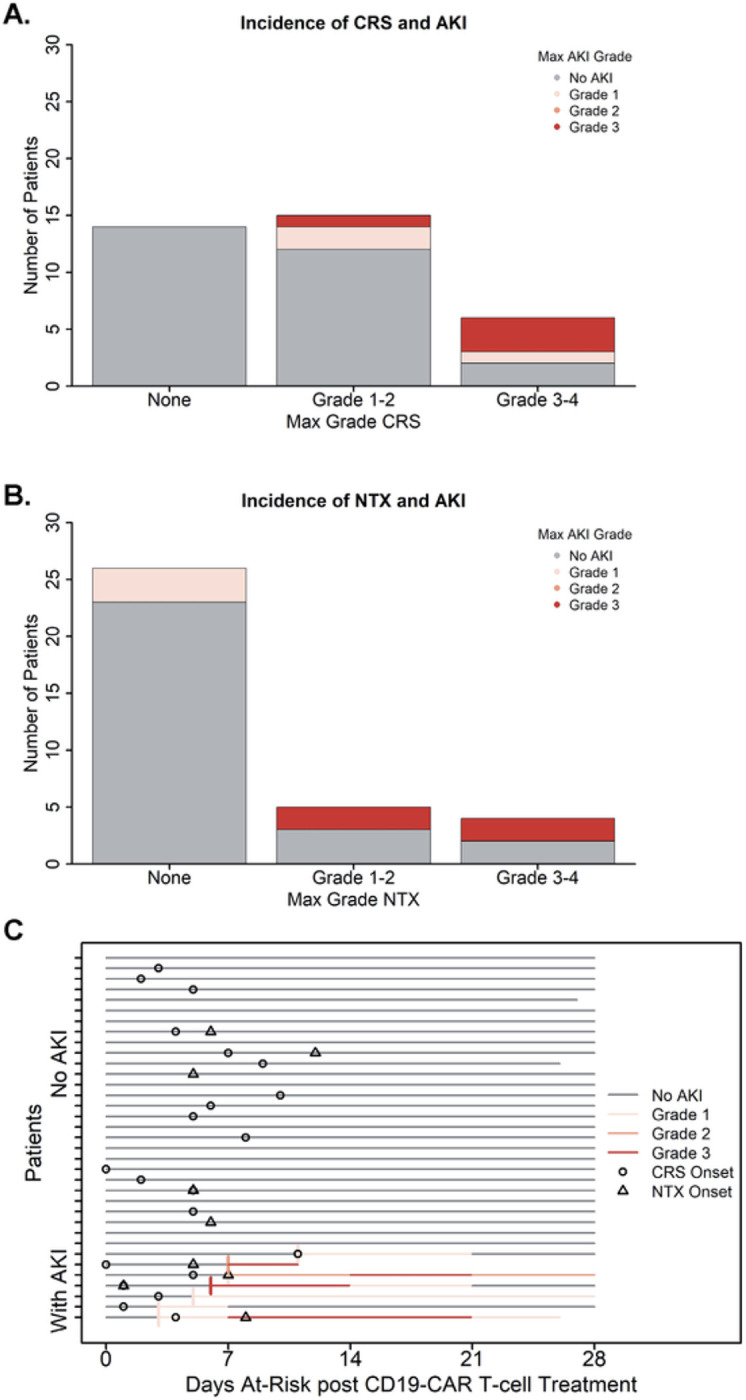
CD19-specific chimeric antigen receptor (CAR) T-cell therapy has shown promising disease responses in patients with high-risk B-cell malignancies. Treatment with CD19-CAR T-cell therapy is also associated with the risk of morbidity and mortality, primarily related to immune-mediated complications (cytokine release syndrome [CRS] and neurotoxicity [NTX]), infections, and end-organ dysfunction. Despite these well-described systemic toxicities, the incidence of post-CAR T-cell therapy acute kidney injury (AKI) in the children, adolescent and young adult (CAYA) patient population is largely unreported. The objectives of this study were to determine the incidence of AKI in CAYA patients with high-risk B-cell malignancies treated with CD19-CAR T-cell therapy, evaluate potential risk factors for developing AKI, and determine patterns of kidney function recovery. In this retrospective analysis of 34 CAYA patients treated with CD19-CAR T-cell at a single institution, we found a cumulative incidence of any grade AKI by day 30 post-infusion of 20% (n=7), with 4 cases being severe AKI (Stage 2-3) and one patient requiring kidney replacement therapy. All episodes of AKI developed within the first 14 days after receiving CAR T-cell therapy and 50% of patients with AKI recovered kidney function to baseline within 30 days post-infusion. No evaluated pre-treatment risk factors were associated with the development of subsequent AKI; there was an association between AKI and CRS and NTX. We conclude that the risk of developing AKI following CD19-CAR T-cell therapy is highest early post-infusion, with most cases of AKI being severe. Although most patients with AKI in our cohort had recovery of kidney function, frequent monitoring to facilitate early recognition and subsequent management of kidney complications after CD19-CAR T-cell therapy may reduce the severity of AKI in the CAYA patient population.
Keywords: CAR T-cell therapy; CD19-CAR; acute kidney injury; pediatric.
Conflict of interest statement
Declaration of Interest: SG consults/consulted for TESSA Therapeutics, TIDAL, Catamaran, and Novartis and is DSMB member of Immatics. SG and RE have patents/patent applications in the fields of T-cell and/or gene therapy for cancer.
Figures

References
-
- Hayden PJ, Roddie C, Bader P, Basak GW, Bonig H, Bonini C et al. (2022) Management of adults and children receiving CAR T-cell therapy: 2021 best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann Oncol 33(3):259–275 - PubMed
-
- Talleur AC, Myers R, Annesley C, Shalabi H (2022) Chimeric Antigen Receptor T-cell Therapy: Current Status and Clinical Outcomes in Pediatric Hematologic Malignancies. Hematol Oncol Clin North Am 36(4):701–727 - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
