

Patisiran Treatment in Patients with Transthyretin Cardiac Amyloidosis
- PMID: 37888916
- PMCID: PMC10757426
- DOI: 10.1056/NEJMoa2300757
Patisiran Treatment in Patients with Transthyretin Cardiac Amyloidosis
Abstract
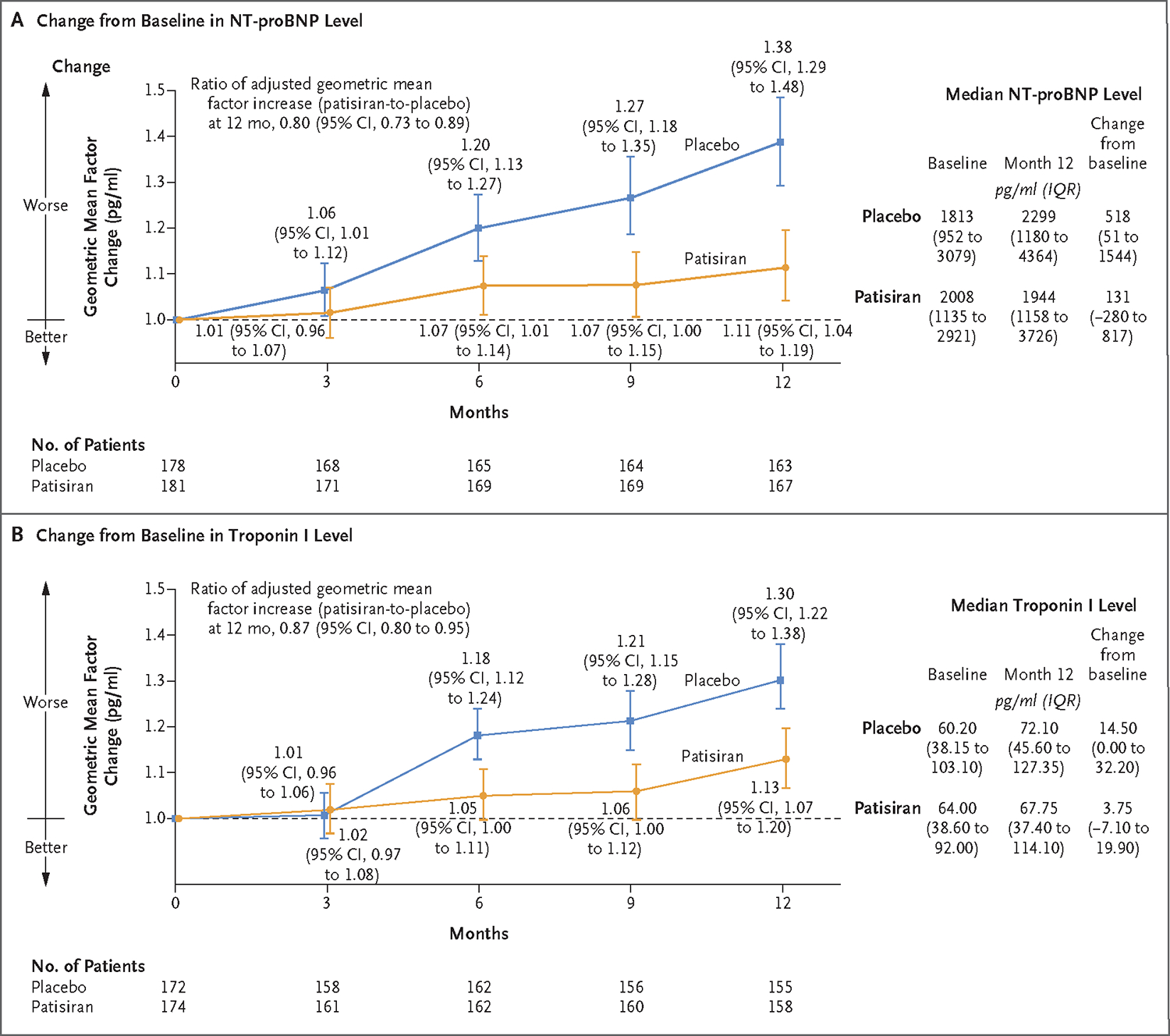
Background: Transthyretin amyloidosis, also called ATTR amyloidosis, is associated with accumulation of ATTR amyloid deposits in the heart and commonly manifests as progressive cardiomyopathy. Patisiran, an RNA interference therapeutic agent, inhibits the production of hepatic transthyretin.
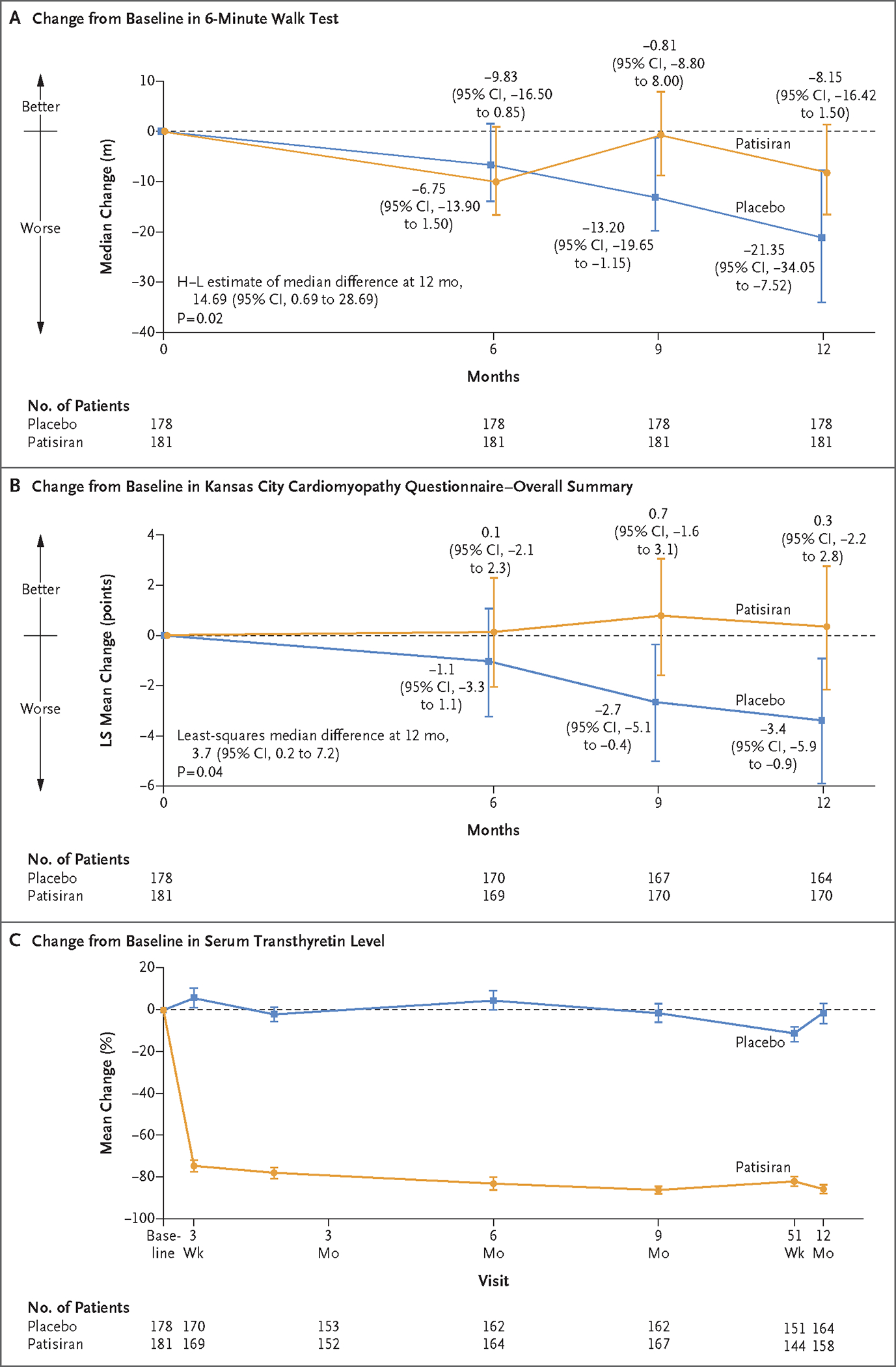
Methods: In this phase 3, double-blind, randomized trial, we assigned patients with hereditary, also known as variant, or wild-type ATTR cardiac amyloidosis, in a 1:1 ratio, to receive patisiran (0.3 mg per kilogram of body weight) or placebo once every 3 weeks for 12 months. A hierarchical procedure was used to test the primary and three secondary end points. The primary end point was the change from baseline in the distance covered on the 6-minute walk test at 12 months. The first secondary end point was the change from baseline to month 12 in the Kansas City Cardiomyopathy Questionnaire-Overall Summary (KCCQ-OS) score (with higher scores indicating better health status). The second secondary end point was a composite of death from any cause, cardiovascular events, and change from baseline in the 6-minute walk test distance over 12 months. The third secondary end point was a composite of death from any cause, hospitalizations for any cause, and urgent heart failure visits over 12 months.
Results: A total of 360 patients were randomly assigned to receive patisiran (181 patients) or placebo (179 patients). At month 12, the decline in the 6-minute walk distance was lower in the patisiran group than in the placebo group (Hodges-Lehmann estimate of median difference, 14.69 m; 95% confidence interval [CI], 0.69 to 28.69; P = 0.02); the KCCQ-OS score increased in the patisiran group and declined in the placebo group (least-squares mean difference, 3.7 points; 95% CI, 0.2 to 7.2; P = 0.04). Significant benefits were not observed for the second secondary end point. Infusion-related reactions, arthralgia, and muscle spasms occurred more often among patients in the patisiran group than among those in the placebo group.
Conclusions: In this trial, administration of patisiran over a period of 12 months resulted in preserved functional capacity in patients with ATTR cardiac amyloidosis. (Funded by Alnylam Pharmaceuticals; APOLLO-B ClinicalTrials.gov number, NCT03997383.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Patisiran is beneficial for the treatment of TTR cardiac amyloidosis.Nat Rev Cardiol. 2024 Jan;21(1):8. doi: 10.1038/s41569-023-00955-2. Nat Rev Cardiol. 2024. PMID: 37932423 No abstract available.
-
Patisiran in Patients with Transthyretin Cardiac Amyloidosis.N Engl J Med. 2024 Jan 18;390(3):286. doi: 10.1056/NEJMc2313408. N Engl J Med. 2024. PMID: 38231632 No abstract available.
-
Patisiran in Patients with Transthyretin Cardiac Amyloidosis. Reply.N Engl J Med. 2024 Jan 18;390(3):286-287. doi: 10.1056/NEJMc2313408. N Engl J Med. 2024. PMID: 38231633 No abstract available.
-
In adults with ATTR cardiac amyloidosis, patisiran reduced decline in functional capacity at 12 mo.Ann Intern Med. 2024 Mar;177(3):JC30. doi: 10.7326/J24-0004. Epub 2024 Mar 5. Ann Intern Med. 2024. PMID: 38437698
References
-
- Adams D, Koike H, Slama M, Coelho T. Hereditary transthyretin amyloidosis: a model of medical progress for a fatal disease. Nat Rev Neurol 2019;15:387–404. - PubMed
-
- Rapezzi C, Quarta CC, Obici L, et al. Disease profile and differential diagnosis of hereditary transthyretin-related amyloidosis with exclusively cardiac phenotype: an Italian perspective. Eur Heart J 2013;34:5 20–8. - PubMed
-
- Coelho T, Maurer MS, Suhr OB. THAOS — the Transthyretin Amyloidosis Outcomes Survey: initial report on clinical manifestations in patients with hereditary and wild-type transthyretin amyloidosis. Curr Med Res Opin 2013;29:63–76. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials