

Use of Telemedicine and Quality of Care Among Medicare Enrollees With Serious Mental Illness
- PMID: 37889483
- PMCID: PMC10611994
- DOI: 10.1001/jamahealthforum.2023.3648
Use of Telemedicine and Quality of Care Among Medicare Enrollees With Serious Mental Illness
Abstract
Importance: During the COVID-19 pandemic, a large fraction of mental health care was provided via telemedicine. The implications of this shift in care for use of mental health service and quality of care have not been characterized.
Objective: To compare changes in care patterns and quality during the first year of the pandemic among Medicare beneficiaries with serious mental illness (schizophrenia or bipolar I disorder) cared for at practices with higher vs lower telemedicine use.
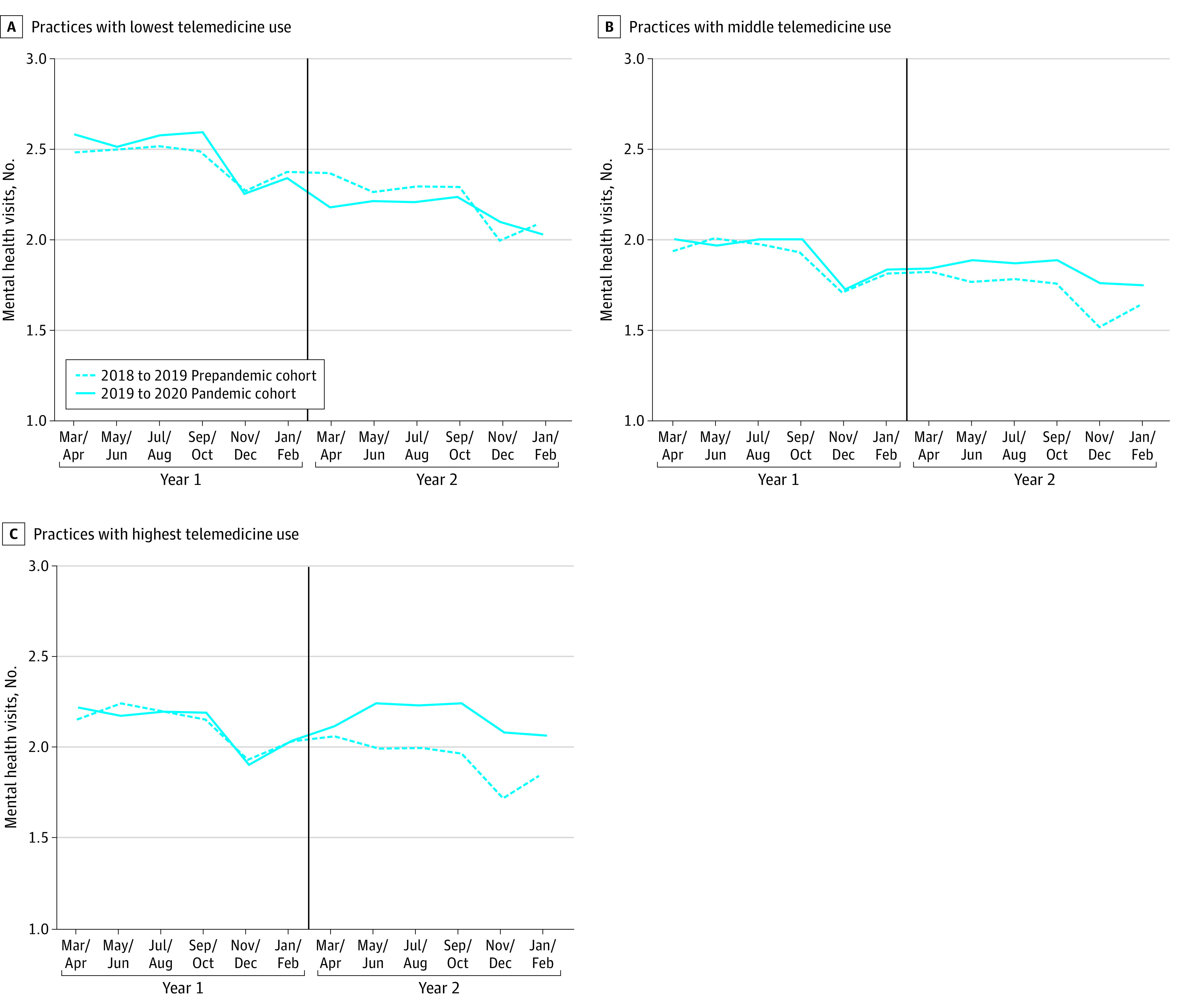
Design, setting, and participants: In this cohort study, Medicare fee-for-service beneficiaries with schizophrenia or bipolar I disorder were attributed to specialty mental health practices that delivered the majority of their mental health care in 2019. Practices were categorized into 3 groups based on the proportion of telemental health visits provided during the first year of the pandemic (March 2020-February 2021): lowest use (0%-49%), middle use (50%-89%), or highest use (90%-100%). Across the 3 groups of practices, differential changes in patient outcomes were calculated from the year before the pandemic started to the year after. These changes were also compared with differential changes from a 2-year prepandemic period. Analyses were conducted in November 2022.
Exposure: Practice-level use of telemedicine during the first year of the COVID-19 pandemic.
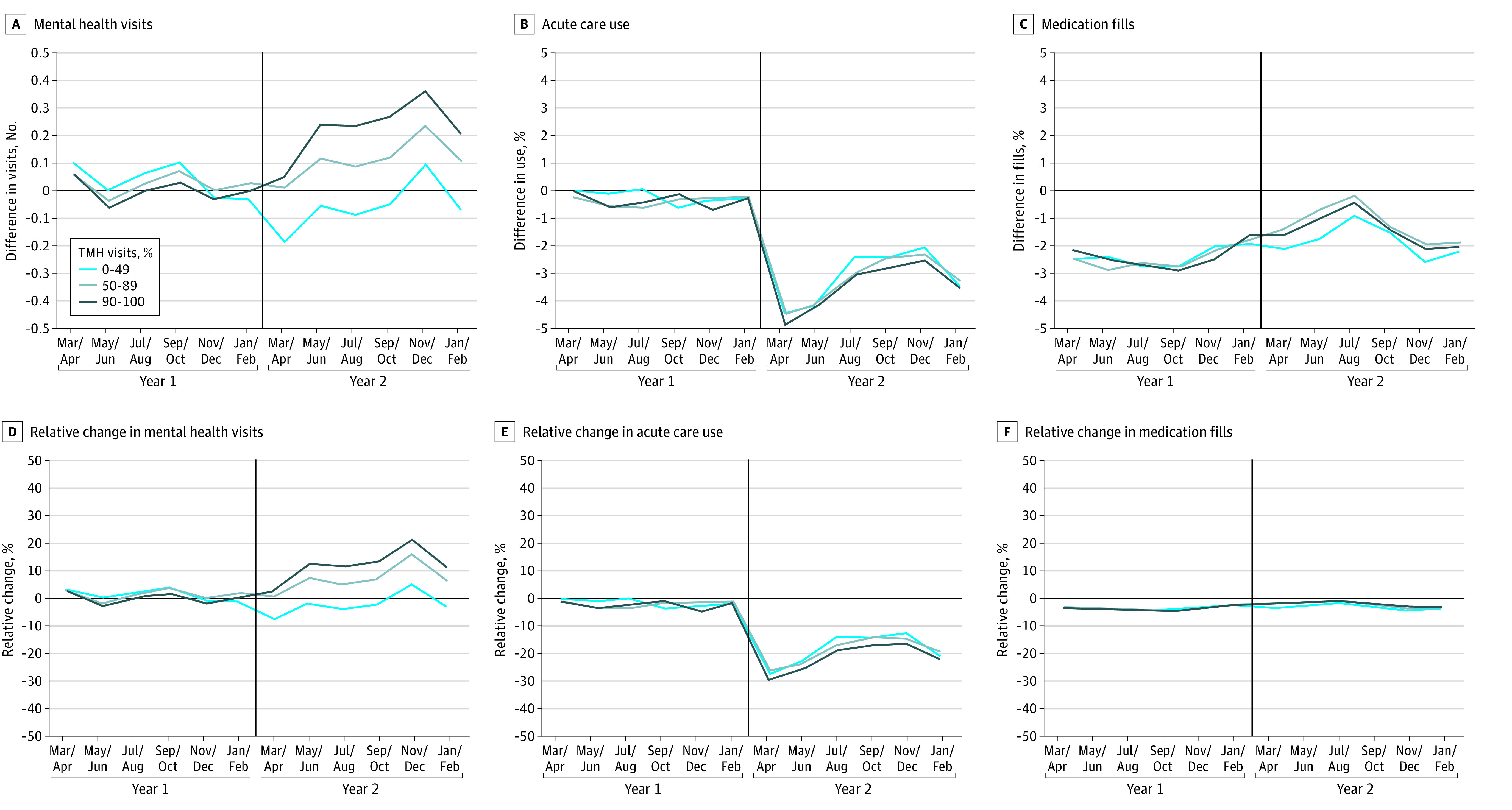
Main outcomes and measures: The primary outcome was the total number of mental health visits (telemedicine plus in-person) per person. Secondary outcomes included the number of acute hospital and emergency department encounters, all-cause mortality, and quality outcomes, including adherence to antipsychotic and mood-stabilizing medications (as measured by the number of months of medication fills) and 7- and 30-day outpatient follow-up rates after discharge for a mental health hospitalization.
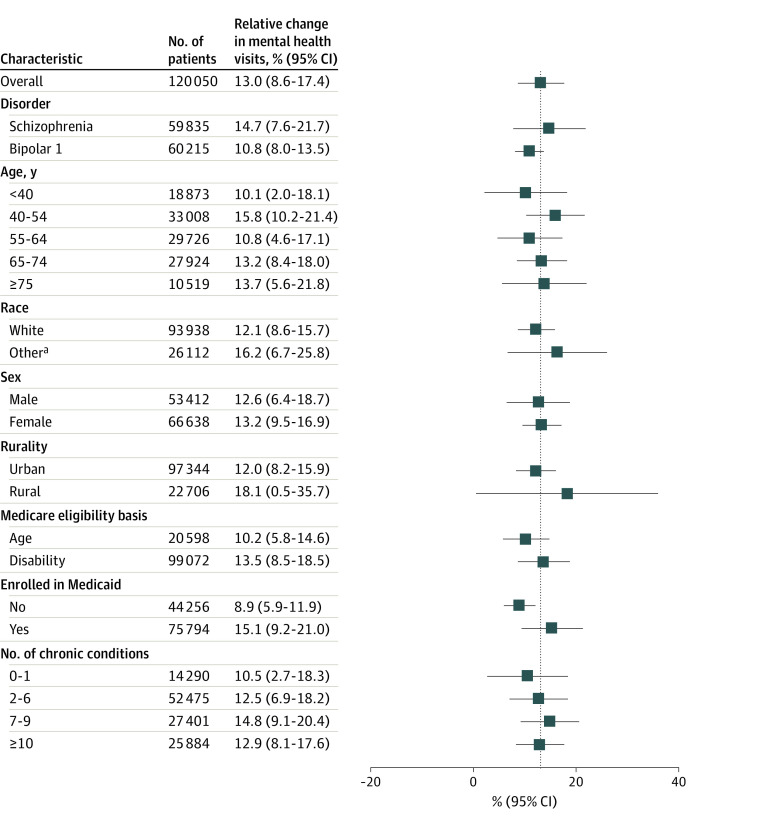
Results: The pandemic cohort included 120 050 Medicare beneficiaries (mean [SD] age, 56.5 [14.5] years; 66 638 females [55.5%]) with serious mental illness. Compared with prepandemic changes and relative to patients receiving care at practices with the lowest telemedicine use: patients receiving care at practices in the middle and highest telemedicine use groups had 1.11 (95% CI, 0.45-1.76) and 1.94 (95% CI, 1.28-2.59) more mental health visits per patient per year (or 7.5% [95% CI, 3.0%-11.9%] and 13.0% [95% CI, 8.6%-17.4%] more mental health visits per year, respectively). Among patients of practices with middle and highest telemedicine use, changes in adherence to antipsychotic and mood-stabilizing medications were -0.4% (95% CI, -1.3% to 0.5%) and -0.1% (95% CI, -1.0% to 0.8%), and hospital and emergency department use for any reason changed by 2.4% (95% CI, -1.5% to 6.2%) and 2.8% (95% CI, -1.2% to 6.8%), respectively. There were no significant differential changes in postdischarge follow-up or mortality rates according to the level of telemedicine use.
Conclusions and relevance: In this cohort study of Medicare beneficiaries with serious mental illness, patients receiving care from practices that had a higher level of telemedicine use during the COVID-19 pandemic had more mental health visits per year compared with prepandemic levels, with no differential changes in other observed quality metrics over the same period.
Conflict of interest statement
Figures
Similar articles
-
Association Between Telemedicine Use in Nonmetropolitan Counties and Quality of Care Received by Medicare Beneficiaries With Serious Mental Illness.JAMA Netw Open. 2022 Jun 1;5(6):e2218730. doi: 10.1001/jamanetworkopen.2022.18730. JAMA Netw Open. 2022. PMID: 35759264 Free PMC article.
-
Disruptions in Care for Medicare Beneficiaries With Severe Mental Illness During the COVID-19 Pandemic.JAMA Netw Open. 2022 Jan 4;5(1):e2145677. doi: 10.1001/jamanetworkopen.2021.45677. JAMA Netw Open. 2022. PMID: 35089352 Free PMC article.
-
Trends in Outpatient Telemedicine Utilization Among Rural Medicare Beneficiaries, 2010 to 2019.JAMA Health Forum. 2021 Oct 15;2(10):e213282. doi: 10.1001/jamahealthforum.2021.3282. eCollection 2021 Oct. JAMA Health Forum. 2021. PMID: 35977168 Free PMC article.
-
Medicare Changes in Response to COVID-19: Unintended Effects for Beneficiaries With Mental Illness or Substance Use Disorders.Psychiatr Serv. 2023 Dec 1;74(12):1285-1288. doi: 10.1176/appi.ps.20220502. Epub 2023 Jun 8. Psychiatr Serv. 2023. PMID: 37287226 Review.
-
The Efficacy of Telemental Health Interventions for Mood Disorders Pre-COVID-19: A Narrative Review.J Behav Health Serv Res. 2024 Jul;51(3):395-420. doi: 10.1007/s11414-024-09884-5. Epub 2024 May 2. J Behav Health Serv Res. 2024. PMID: 38698193 Free PMC article. Review.
Cited by
-
Accountable Care Organizations, Mental Health, and Aging in the New Era of Digital Health.Public Policy Aging Rep. 2024 Apr 26;34(2):54-58. doi: 10.1093/ppar/prae003. eCollection 2024. Public Policy Aging Rep. 2024. PMID: 38946715 Free PMC article. No abstract available.
-
Gaps in psychiatric care before and after the COVID-19 pandemic among patients with depression using electronic health records.Psychiatry Res. 2025 Feb;344:116354. doi: 10.1016/j.psychres.2025.116354. Epub 2025 Jan 6. Psychiatry Res. 2025. PMID: 39799819
-
Differential impacts of the COVID-19 pandemic on mental health service access among Medicaid-enrolled individuals.Health Aff Sch. 2024 Aug 20;2(9):qxae104. doi: 10.1093/haschl/qxae104. eCollection 2024 Sep. Health Aff Sch. 2024. PMID: 39220582 Free PMC article.
-
Policy Changes to Promote Better Quality of Life for People with Serious Mental Illness Living in U.S. Nursing Homes.Public Policy Aging Rep. 2024 May 6;34(2):65-70. doi: 10.1093/ppar/prae004. eCollection 2024. Public Policy Aging Rep. 2024. PMID: 38946714 Free PMC article. No abstract available.
-
Telemedicine Compared to Office-Based Care of Patients With Cardiac Symptoms: Treatment and Outcomes.JACC Adv. 2024 Oct 18;3(11):101353. doi: 10.1016/j.jacadv.2024.101353. eCollection 2024 Nov. JACC Adv. 2024. PMID: 39469609 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
