

A Novel Nomogram Based on Quantitative MRI and Clinical Features for the Prediction of Neonatal Intracranial Hypertension
- PMID: 37892245
- PMCID: PMC10605298
- DOI: 10.3390/children10101582
A Novel Nomogram Based on Quantitative MRI and Clinical Features for the Prediction of Neonatal Intracranial Hypertension
Abstract
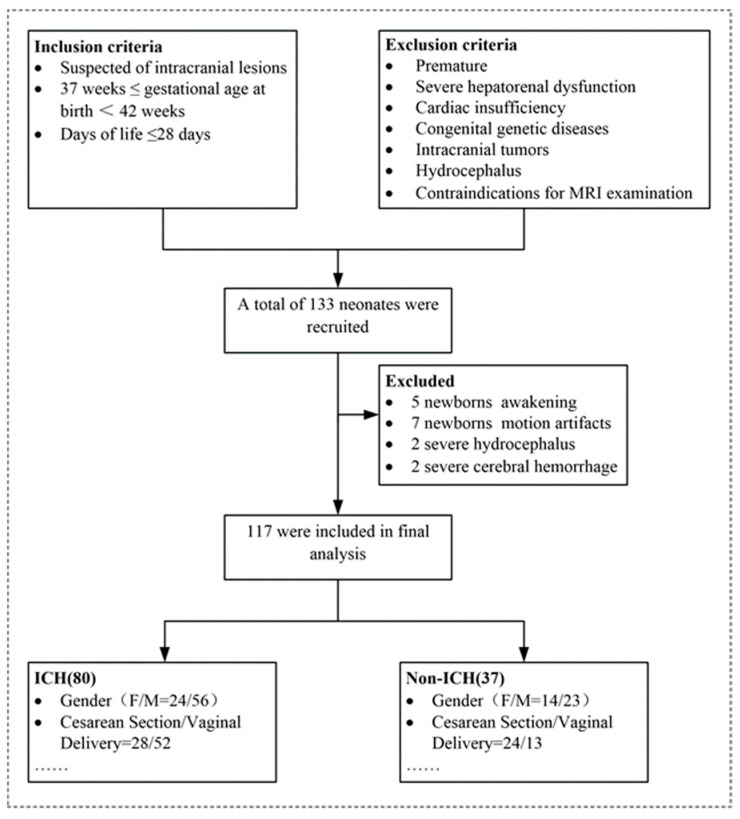
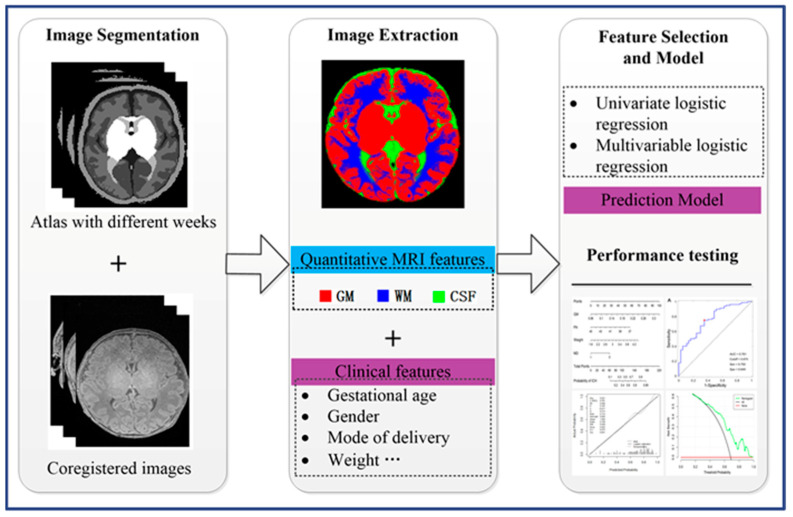
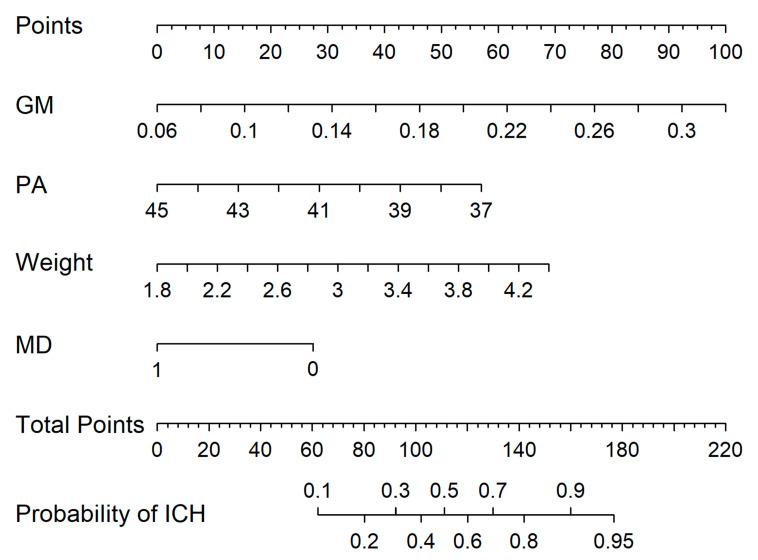
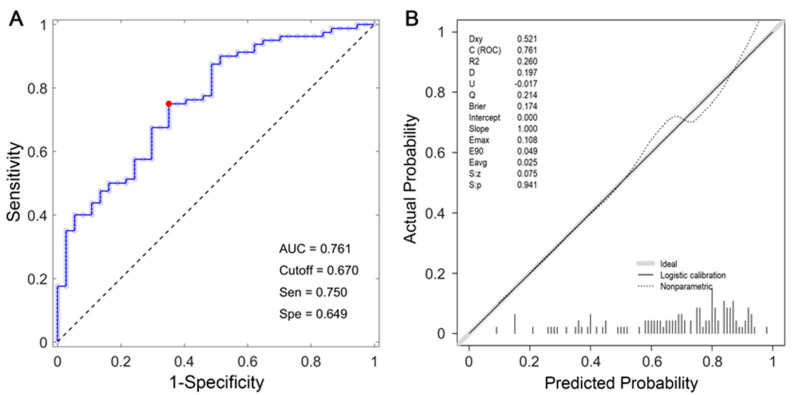
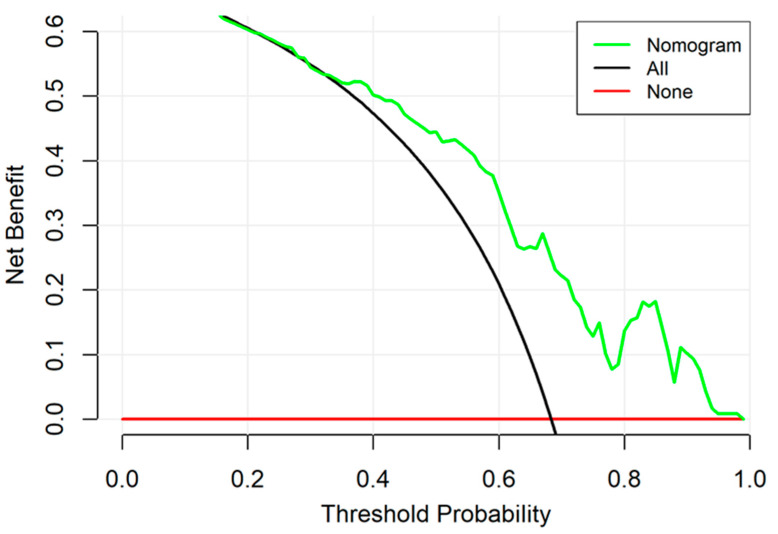
Intracranial hypertension (ICH) is a serious threat to the health of neonates. However, early and accurate diagnosis of neonatal intracranial hypertension remains a major challenge in clinical practice. In this study, a predictive model based on quantitative magnetic resonance imaging (MRI) data and clinical parameters was developed to identify neonates with a high risk of ICH. Newborns who were suspected of having intracranial lesions were included in our study. We utilized quantitative MRI to obtain the volumetric data of gray matter, white matter, and cerebrospinal fluid. After the MRI examination, a lumbar puncture was performed. The nomogram was constructed by incorporating the volumetric data and clinical features by multivariable logistic regression. The performance of the nomogram was evaluated by discrimination, calibration curve, and decision curve. Clinical parameters and volumetric quantitative MRI data, including postmenstrual age (p = 0.06), weight (p = 0.02), mode of delivery (p = 0.01), and gray matter volume (p = 0.003), were included in and significantly associated with neonatal intracranial hypertension risk. The nomogram showed satisfactory discrimination, with an area under the curve of 0.761. Our results demonstrated that decision curve analysis had promising clinical utility of the nomogram. The nomogram, incorporating clinical and quantitative MRI features, provided an individualized prediction of neonatal intracranial hypertension risk and facilitated decision making guidance for the early diagnosis and treatment for neonatal ICH. External validation from studies using a larger sample size before implementation in the clinical decision-making process is needed.
Keywords: intracranial hypertension; magnetic resonance imaging; neonate; prediction; volumetric segmentation.
Conflict of interest statement
None of the authors have a financial interest to declare in relation to the content of this article.
Figures
References
-
- Dessardo N.S., Dessardo S., Sasso A., Sarunic A.V., Dezulovic M.S. Pediatric idiopathic intracranial hypertension: Clinical and demographic features. Coll. Antropol. 2010;34((Suppl. S2)):217–221. - PubMed
-
- Gordon K. Pediatric pseudotumor cerebri: Descriptive epidemiology. Can. J. Neurol. Sci. 1997;24:219–221. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
