

Caring for Infants with Robin Sequence Treated with the Tübingen Palatal Plate: A Review of Personal Practice
- PMID: 37892291
- PMCID: PMC10605622
- DOI: 10.3390/children10101628
Caring for Infants with Robin Sequence Treated with the Tübingen Palatal Plate: A Review of Personal Practice
Abstract
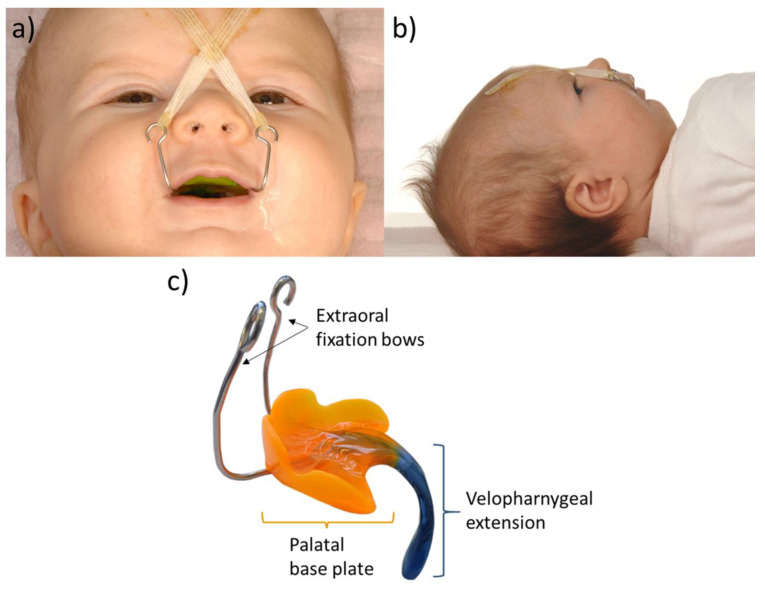
The Tübingen Palatal Plate (TPP) is a minimally invasive yet highly effective functional orthodontic treatment for upper airway obstruction in infants with Robin Sequence (RS). It consists of a palatal plate to cover the cleft and a velar extension that shifts the root of the tongue forward. We review our practical experience with this approach. First, upon admission, our local orthodontists perform an (3-D) intraoral scan of the maxilla. Based on the scan data, the TPP is manufactured in a semi-digital workflow. The length and angulation of its extension is checked via awake laryngoscopy and the effectiveness confirmed by a sleep study. Plates are kept in place by adhesive cream. When inserting the TPP, the tip of the tongue must be visible. Next, metal fixation bows should be secured to the forehead using tape and elastic bands. Plates are removed daily for cleaning, and the oral mucosa is then checked for pressure marks. Feeding training (initially only via finger feeding) may even start before plate insertion. Breathing often normalizes immediately once the plate is inserted. For isolated RS, we have never had to perform a tracheostomy. This has largely been possible through our highly dedicated and competent team, particularly the nursing staff, and the early involvement of parents.
Keywords: Pierre Robin sequence; cleft palate; feeding; functional treatment; intraoral scanning; mandibular retrognathia; upper airway obstruction.
Conflict of interest statement
The authors declare no conflict of interest. No external funding was received for this work.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
