

Advances in Therapies to Treat Neonatal Hypoxic-Ischemic Encephalopathy
- PMID: 37892791
- PMCID: PMC10607511
- DOI: 10.3390/jcm12206653
Advances in Therapies to Treat Neonatal Hypoxic-Ischemic Encephalopathy
Abstract
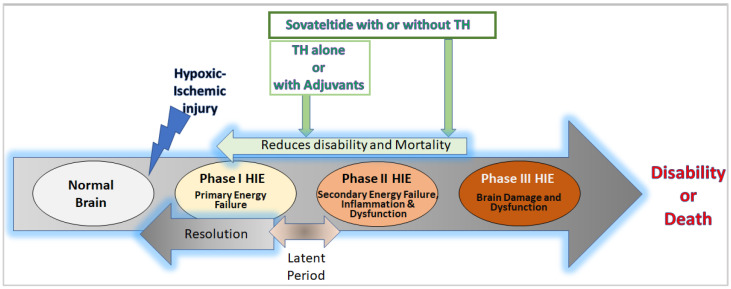
Neonatal hypoxic-ischemic encephalopathy (HIE) is a condition that results in brain damage in newborns due to insufficient blood and oxygen supply during or after birth. HIE is a major cause of neurological disability and mortality in newborns, with over one million neonatal deaths occurring annually worldwide. The severity of brain injury and the outcome of HIE depend on several factors, including the cause of oxygen deprivation, brain maturity, regional blood flow, and maternal health conditions. HIE is classified into mild, moderate, and severe categories based on the extent of brain damage and resulting neurological issues. The pathophysiology of HIE involves different phases, including the primary phase, latent phase, secondary phase, and tertiary phase. The primary and secondary phases are characterized by episodes of energy and cell metabolism failures, increased cytotoxicity and apoptosis, and activated microglia and inflammation in the brain. A tertiary phase occurs if the brain injury persists, characterized by reduced neural plasticity and neuronal loss. Understanding the cellular and molecular aspects of the different phases of HIE is crucial for developing new interventions and therapeutics. This review aims to discuss the pathophysiology of HIE, therapeutic hypothermia (TH), the only approved therapy for HIE, ongoing developments of adjuvants for TH, and potential future drugs for HIE.
Keywords: IRL-1620; PMZ 1620; cerebral palsy; endothelin B receptors; hypoxia; ischemia; neonates; neurogenesis; oxidative stress; perinatal asphyxia; regeneration; sovateltide; stem/progenitor cells.
Conflict of interest statement
A.G. is a Pharmazz, Inc. employee and has issued and pending patents related to the studies described in this review. A.K.R. is a Pharmazz Inc. employee and declares no other competing interest.
Figures
References
-
- Yokomaku D., Numakawa T., Numakawa Y., Suzuki S., Matsumoto T., Adachi N., Nishio C., Taguchi T., Hatanaka H. Estrogen enhances depolarization-induced glutamate release through activation of phosphatidylinositol 3-kinase and mitogen-activated protein kinase in cultured hippocampal neurons. Mol. Endocrinol. 2003;17:831–844. doi: 10.1210/me.2002-0314. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
