

Prevalence and Impact of Cerebral Microbleeds on Clinical and Safety Outcomes in Acute Ischaemic Stroke Patients Receiving Reperfusion Therapy: A Systematic Review and Meta-Analysis
- PMID: 37893237
- PMCID: PMC10604359
- DOI: 10.3390/biomedicines11102865
Prevalence and Impact of Cerebral Microbleeds on Clinical and Safety Outcomes in Acute Ischaemic Stroke Patients Receiving Reperfusion Therapy: A Systematic Review and Meta-Analysis
Abstract
Background: Cerebral microbleeds (CMBs), a notable neuroimaging finding often associated with cerebral microangiopathy, demonstrate a heightened prevalence in patients diagnosed with acute ischemic stroke (AIS), which is in turn linked to less favourable clinical prognoses. Nevertheless, the exact prevalence of CMBs and their influence on post-reperfusion therapy outcomes remain inadequately elucidated.
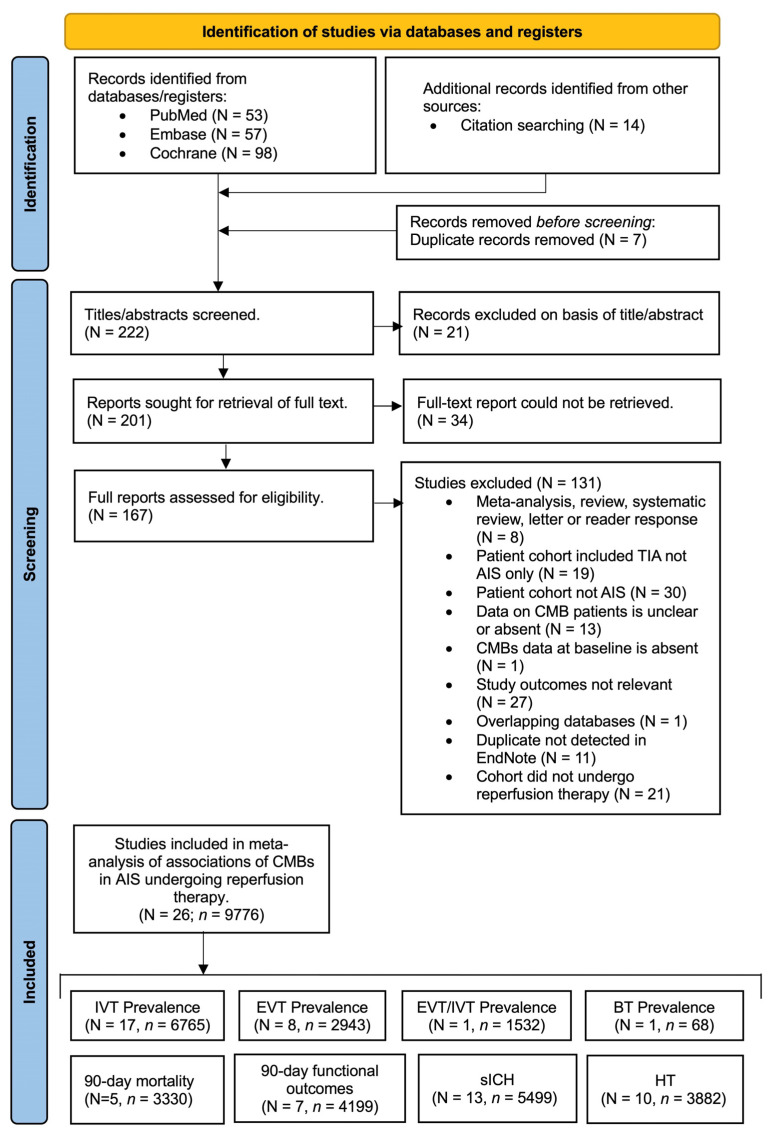
Materials and methods: Through systematic searches of PubMed, Embase and Cochrane databases, studies were identified adhering to specific inclusion criteria: (a) AIS patients, (b) age ≥ 18 years, (c) CMBs at baseline, (d) availability of comparative data between CMB-positive and CMB-negative groups, along with relevant post-reperfusion therapy outcomes. The data extracted were analysed using forest plots of odds ratios, and random-effects modelling was applied to investigate the association between CMBs and symptomatic intracerebral haemorrhage (sICH), haemorrhagic transformation (HT), 90-day functional outcomes, and 90-day mortality post-reperfusion therapy.
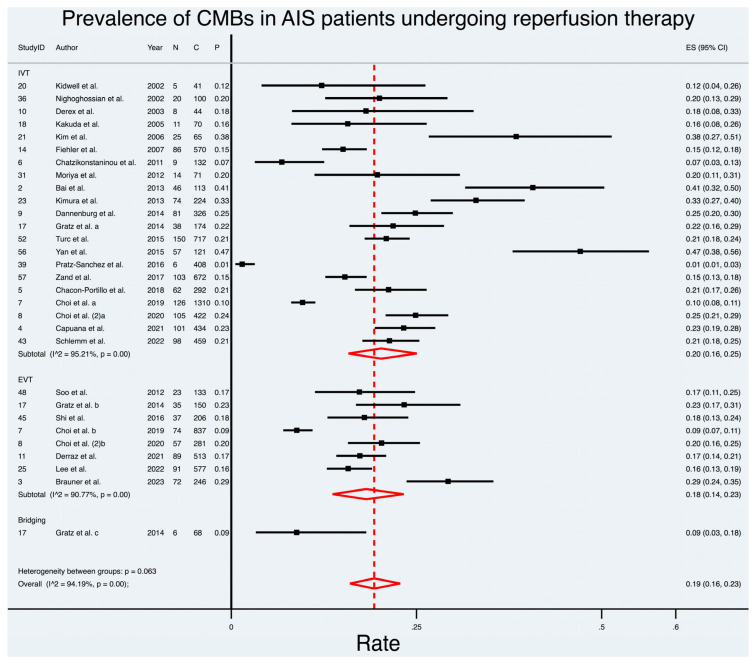
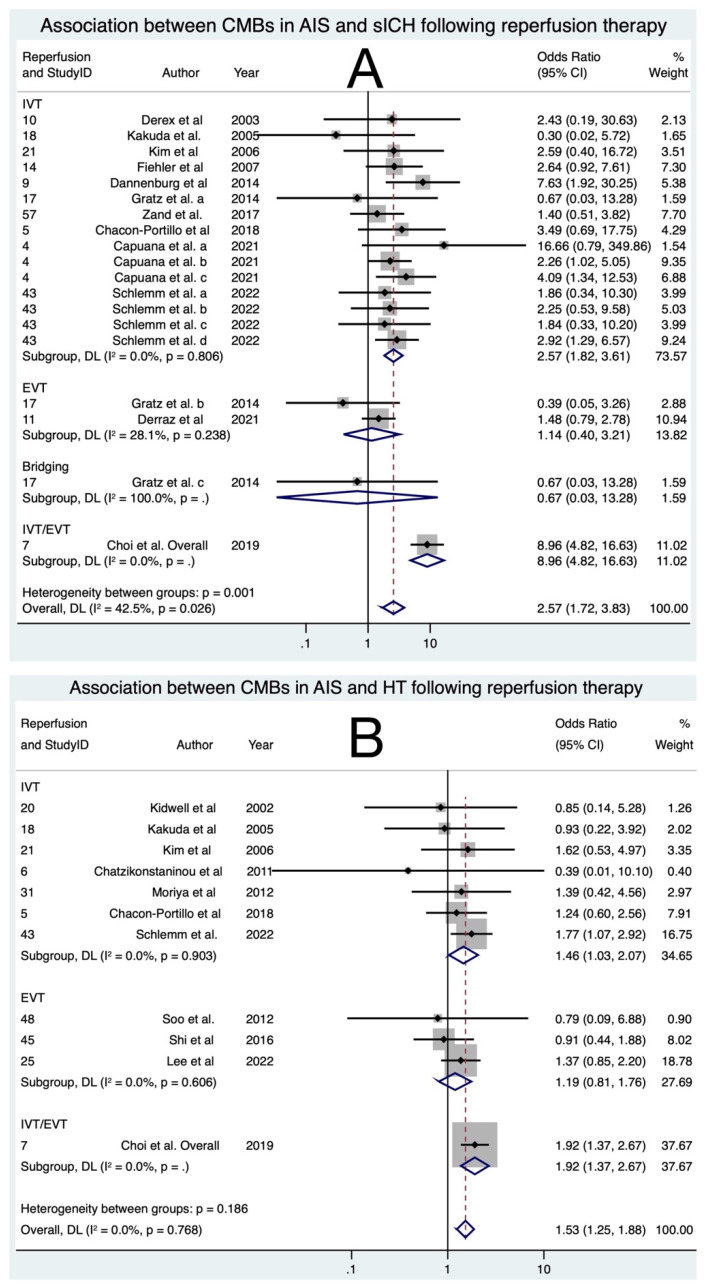
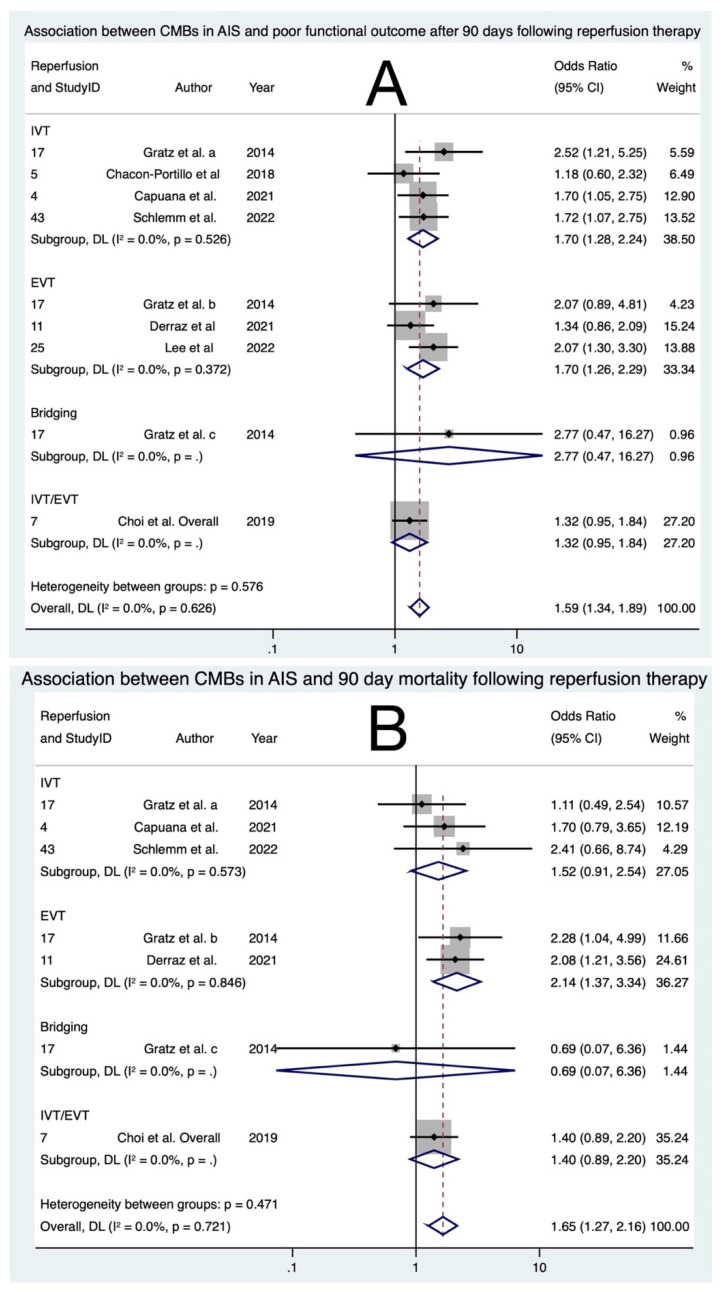
Results: In a total cohort of 9776 AIS patients who underwent reperfusion therapy, 1709 had CMBs, with a pooled prevalence of 19% (ES 0.19; 95% CI: 0.16, 0.23, p < 0.001). CMBs significantly increased the odds of sICH (OR 2.57; 95% CI: 1.72; 3.83; p < 0.0001), HT (OR 1.53; 95% CI: 1.25; 1.88; p < 0.0001), as well as poor functional outcomes at 90 days (OR 1.59; 95% CI: 1.34; 1.89; p < 0.0001) and 90-day mortality (OR 1.65; 95% CI: 1.27; 2.16; p < 0.0001), relative to those without CMBs, in AIS patients undergoing reperfusion therapy (encompassing intravenous thrombolysis [IVT], endovascular thrombectomy [EVT], either IVT or EVT, and bridging therapy). Variations in the level of association can be observed among different subgroups of reperfusion therapy.
Conclusions: This meta-analysis underscores a significant association between CMBs and adverse postprocedural safety outcomes encompassing sICH, HT, poor functional outcome, and increased mortality in AIS patients undergoing reperfusion therapy. The notable prevalence of CMBs in both the overall AIS population and those undergoing reperfusion therapy emphasizes their importance in post-stroke prognostication.
Keywords: cerebral microbleeds; haemorrhage; meta-analysis; prevalence; reperfusion therapy; stroke.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
