

Recent Advances and Adaptive Strategies in Image Guidance for Cervical Cancer Radiotherapy
- PMID: 37893453
- PMCID: PMC10608436
- DOI: 10.3390/medicina59101735
Recent Advances and Adaptive Strategies in Image Guidance for Cervical Cancer Radiotherapy
Abstract
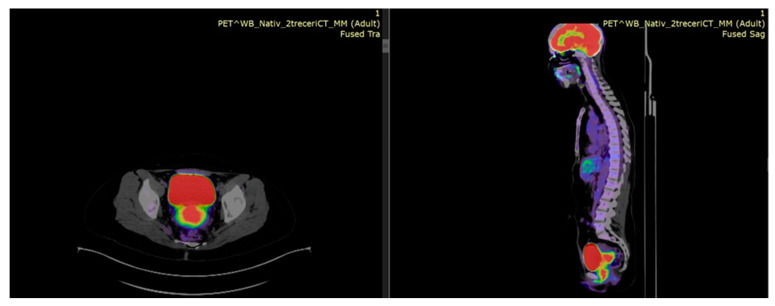
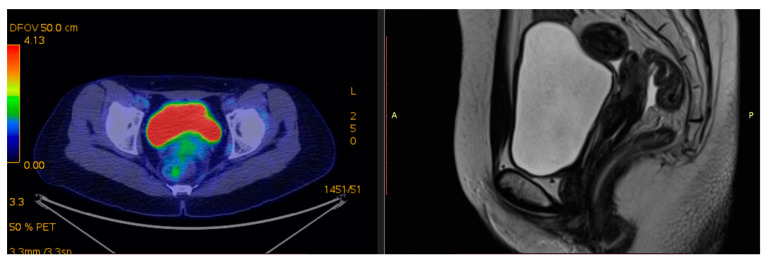
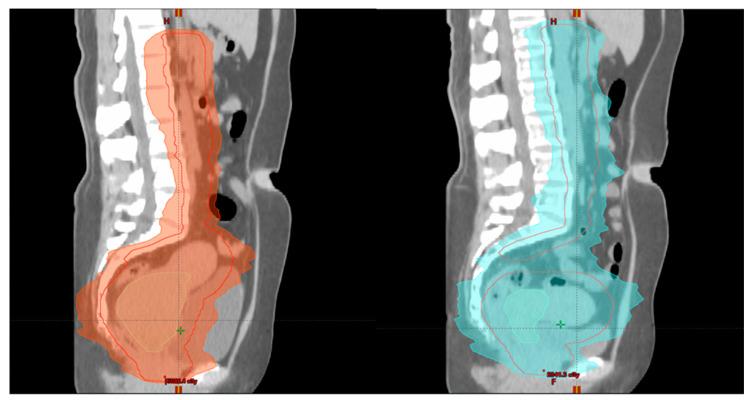
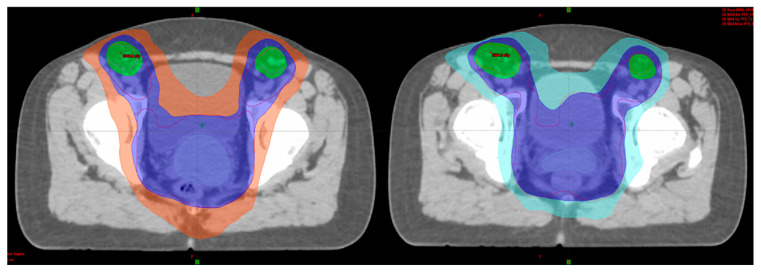
The standard of care for locally advanced cervical cancer is external beam radiotherapy (EBRT) with simultaneous chemotherapy followed by an internal radiation boost. New imaging methods such as positron-emission tomography and magnetic resonance imaging have been implemented into daily practice for better tumor delineation in radiotherapy planning. The method of delivering radiation has changed with technical advances in qualitative imaging and treatment delivery. Image-guided radiotherapy (IGRT) plays an important role in minimizing treatment toxicity of pelvic radiation and provides a superior conformality for sparing the organs at risk (OARs) such as bone marrow, bowel, rectum, and bladder. Similarly, three-dimensional image-guided adaptive brachytherapy (3D-IGABT) with computed tomography (CT) or magnetic resonance imaging (MRI) has been reported to improve target coverage and reduce the dose to normal tissues. Brachytherapy is a complementary part of radiotherapy treatment for cervical cancer and, over the past 20 years, 3D-image-based brachytherapy has rapidly evolved and established itself as the gold standard. With new techniques and adaptive treatment in cervical cancer, the concept of personalized medicine is introduced with an enhanced comprehension of the therapeutic index not only in terms of volume (three-dimensional) but during treatment too (four-dimensional). Current data show promising results with integrated IGRT and IGABT in clinical practice and, therefore, better local control and overall survival while reducing treatment-related morbidity. This review gives an overview of the substantial impact that occurred in the progress of image-guided adaptive external beam radiotherapy and brachytherapy.
Keywords: ART; IGRT; cervix cancer; external beam radiotherapy; image-guided brachytherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Long term experience with 3D image guided brachytherapy and clinical outcome in cervical cancer patients.Radiother Oncol. 2016 Sep;120(3):447-454. doi: 10.1016/j.radonc.2016.04.016. Epub 2016 May 2. Radiother Oncol. 2016. PMID: 27157510
-
MRI-guided adaptive brachytherapy for locally advanced cervix cancer: Treatment outcomes from a single institution in Hong Kong.Brachytherapy. 2019 Mar-Apr;18(2):171-179. doi: 10.1016/j.brachy.2018.11.007. Epub 2018 Dec 21. Brachytherapy. 2019. PMID: 30581053
-
Effect of bladder distension on doses to organs at risk in Pulsed-Dose-Rate 3D image-guided adaptive brachytherapy for locally advanced cervical cancer.Brachytherapy. 2017 Sep-Oct;16(5):976-980. doi: 10.1016/j.brachy.2017.06.003. Epub 2017 Jul 8. Brachytherapy. 2017. PMID: 28694116
-
High-Dose-Rate Three-Dimensional Image-Guided Adaptive Brachytherapy (3D IGABT) for Locally Advanced Cervical Cancer (LACC): A Narrative Review on Imaging Modality and Clinical Evidence.Curr Oncol. 2023 Dec 21;31(1):50-65. doi: 10.3390/curroncol31010004. Curr Oncol. 2023. PMID: 38275830 Free PMC article. Review.
-
Advances in Radiation Oncology for the Treatment of Cervical Cancer.Curr Oncol. 2022 Feb 9;29(2):928-944. doi: 10.3390/curroncol29020079. Curr Oncol. 2022. PMID: 35200578 Free PMC article. Review.
Cited by
-
The Impact of Dual and Triple Energy Window Scatter Correction on I-123 Postsurgical Thyroid SPECT/CT Imaging Using a Phantom with Small Sizes of Thyroid Remnants.Life (Basel). 2024 Jan 11;14(1):113. doi: 10.3390/life14010113. Life (Basel). 2024. PMID: 38255728 Free PMC article.
-
Initial needle tracking with the first standalone combined infrared camera - CT system for brachytherapy-analysis of tracking accuracy and uncertainties.Strahlenther Onkol. 2025 Feb;201(2):163-172. doi: 10.1007/s00066-024-02253-3. Epub 2024 Jul 5. Strahlenther Onkol. 2025. PMID: 38967820 Free PMC article.
-
Radiation Promotes Acute and Chronic Damage to Adipose Tissue.Int J Mol Sci. 2025 Jun 12;26(12):5626. doi: 10.3390/ijms26125626. Int J Mol Sci. 2025. PMID: 40565100 Free PMC article.
-
Adaptive Approach to Treating Cervical Cancer in a Patient With Dramatic Uterine Movement.Cureus. 2024 Nov 3;16(11):e72938. doi: 10.7759/cureus.72938. eCollection 2024 Nov. Cureus. 2024. PMID: 39498428 Free PMC article.
-
A comparative analysis of toxicity and treatment outcomes of adaptive radiotherapy and intensity-modulated radiotherapy in cervical cancer.Sci Rep. 2025 Jan 10;15(1):1609. doi: 10.1038/s41598-024-85074-9. Sci Rep. 2025. PMID: 39794450 Free PMC article.
References
-
- Walboomers J.M.M., Jacobs M.V., Manos M.M., Bosch F.X., Kummer J.A., Shah K.V., Snijders P.J., Peto J., Meijer C.J., Muñoz N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999;189:12–19. doi: 10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F. - DOI - PubMed
