

A C-Arm-Free Minimally Invasive Technique for Spinal Surgery: Cervical and Thoracic Spine
- PMID: 37893497
- PMCID: PMC10607948
- DOI: 10.3390/medicina59101779
A C-Arm-Free Minimally Invasive Technique for Spinal Surgery: Cervical and Thoracic Spine
Abstract
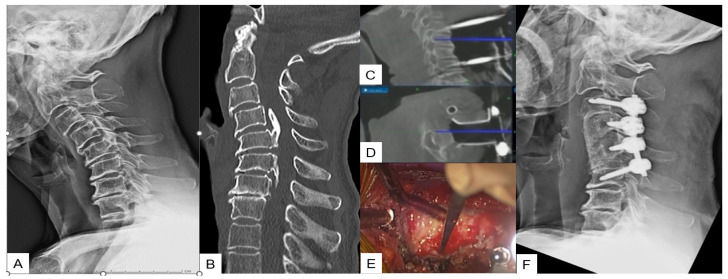
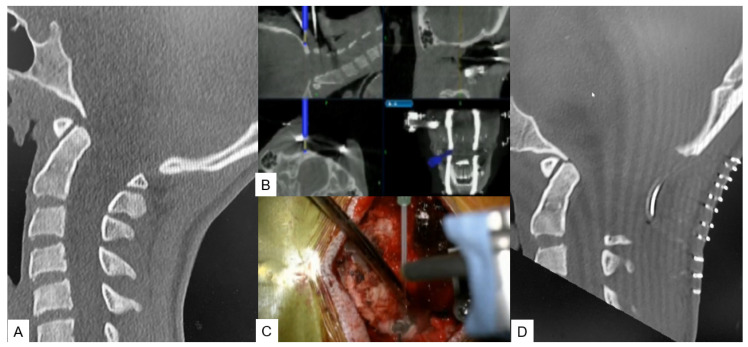
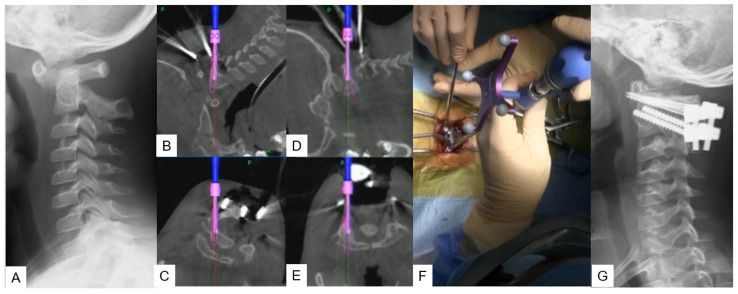
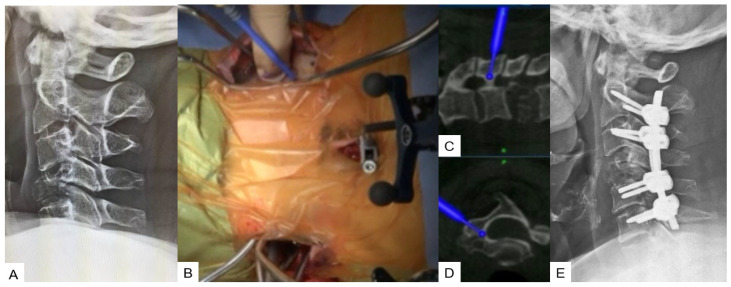
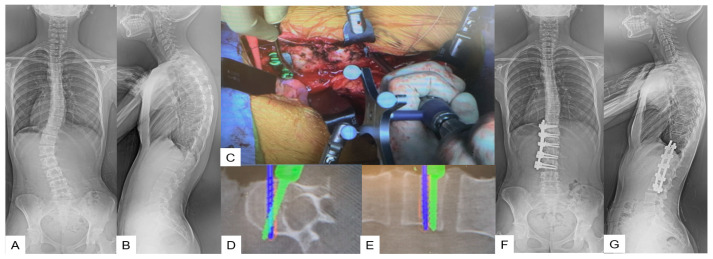
Background and Objectives: C-arm-free MIS techniques can offer significantly reduced rates of postoperative complications such as inadequate decompression, blood loss, and instrumentation misplacement. Another advantageous long-term aspect is the notably diminished exposure to radiation, which is known to cause malignant changes. This study emphasizes that, in some cases of spinal conditions that require a procedural intervention, C-arm-free MIS techniques hold stronger indications than open surgeries guided by image intensifiers. Materials and Methods: This study includes a retrospective analysis and review of various cervical and thoracic spinal procedures, performed in our hospital, applying C-arm-free techniques. The course of this study explains the basic steps of the procedures and demonstrates postoperative and intraoperative results. For anterior cervical surgery, we performed OPLL resection, while for posterior cervical surgery, we performed posterior fossa decompression for Chiari malformation, minimally invasive cervical pedicle screw fixation (MICEPS), and modified Goel technique with C1 lateral mass screw for atlantoaxial subluxation. Regarding the thoracic spine, we performed anterior correction for Lenke type 5 scoliosis and transdiscal screw fixation for diffuse idiopathic skeletal hyperostosis fractures. Results: C-arm-free techniques are safe procedures that provide precise and high-quality postoperative results by offering sufficient spine alignment and adequate decompression depending on the case. Navigation can offer significant assistance in the absence of normal anatomical landmarks, yet the surgeon should always appraise the quality of the information received from the software. Conclusions: Navigated C-arm-free techniques are safe and precise procedures implemented in the treatment of surgically demanding conditions. They can significantly increase accuracy while decreasing operative time. They represent the advancement in the field of spine surgery and are hailed as the future of the same.
Keywords: C-arm free; adult spinal deformity; lateral access spine surgery; minimally invasive spine surgery; oblique lumbar interbody fusion.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Complication rates associated with open versus percutaneous pedicle screw instrumentation among patients undergoing minimally invasive interbody fusion for adult spinal deformity.Neurosurg Focus. 2017 Dec;43(6):E7. doi: 10.3171/2017.8.FOCUS17479. Neurosurg Focus. 2017. PMID: 29191098
-
Minimally invasive scoliosis surgery assisted by O-arm navigation for Lenke Type 5C adolescent idiopathic scoliosis: a comparison with standard open approach spinal instrumentation.J Neurosurg Pediatr. 2017 Apr;19(4):472-478. doi: 10.3171/2016.11.PEDS16412. Epub 2017 Feb 10. J Neurosurg Pediatr. 2017. PMID: 28186473
-
Minimally invasive lateral interbody fusion for the treatment of rostral adjacent-segment lumbar degenerative stenosis without supplemental pedicle screw fixation.J Neurosurg Spine. 2014 Dec;21(6):861-6. doi: 10.3171/2014.8.SPINE13841. Epub 2014 Oct 10. J Neurosurg Spine. 2014. PMID: 25303619
-
[Relevance of spinal navigation in reconstructive surgery of the cervical spine].Orthopade. 2018 Jun;47(6):518-525. doi: 10.1007/s00132-018-3568-x. Orthopade. 2018. PMID: 29663038 Review. German.
Cited by
-
Navigation-Guided C-arm-Free Minimally Invasive Transforaminal Lumbar Interbody Fusion: A Comparative Study of Cage Orientation and Screw Insertion Accuracy Against the Conventional C-arm-Assisted Technique.Cureus. 2024 Aug 3;16(8):e66070. doi: 10.7759/cureus.66070. eCollection 2024 Aug. Cureus. 2024. PMID: 39224725 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
