

Pityriasis Versicolor-A Narrative Review on the Diagnosis and Management
- PMID: 37895478
- PMCID: PMC10608716
- DOI: 10.3390/life13102097
Pityriasis Versicolor-A Narrative Review on the Diagnosis and Management
Abstract
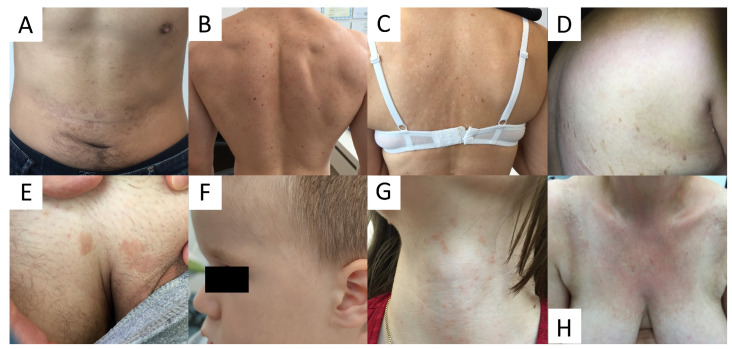
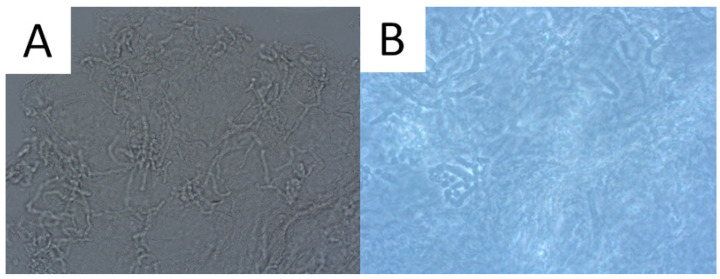
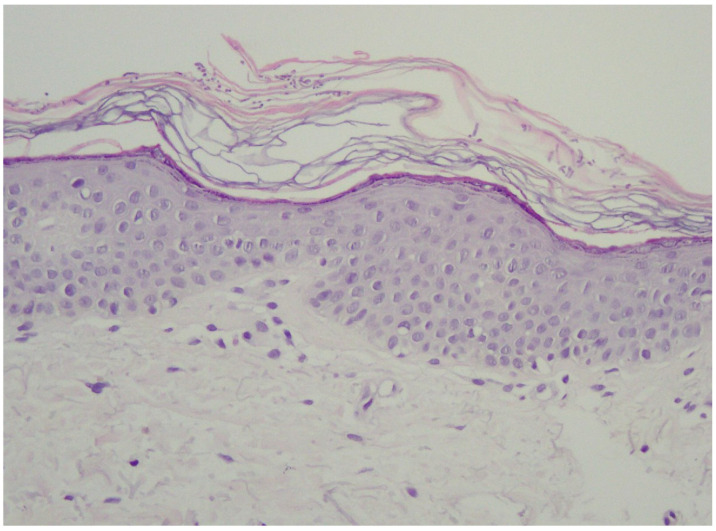
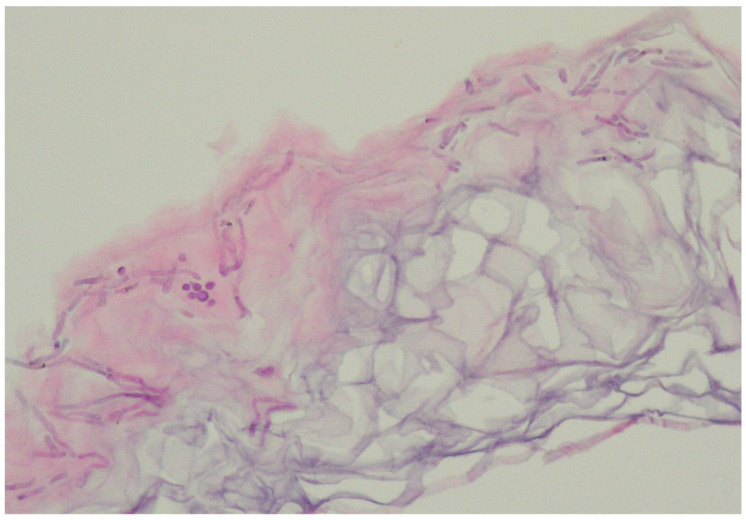
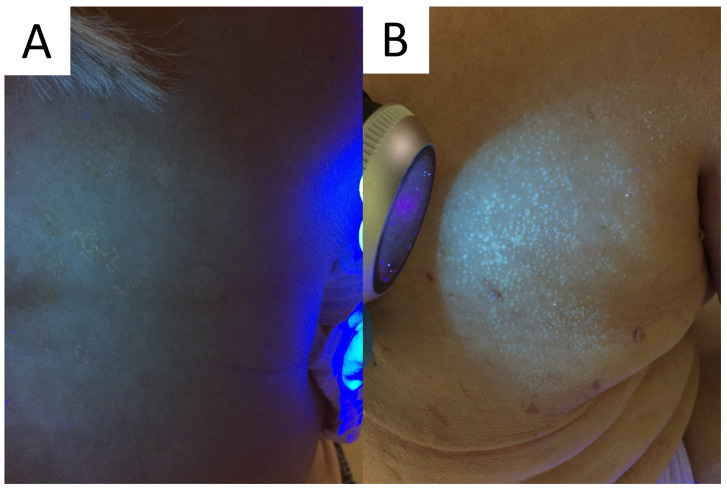
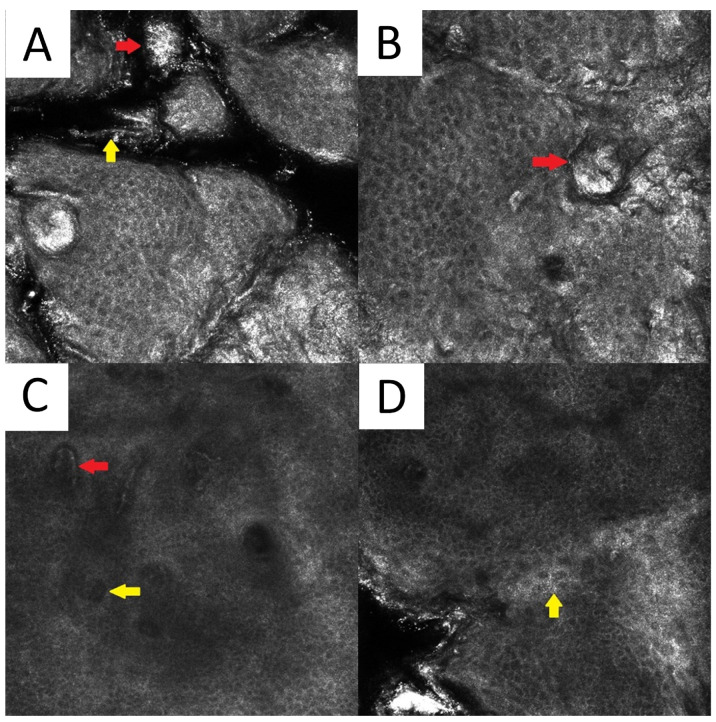
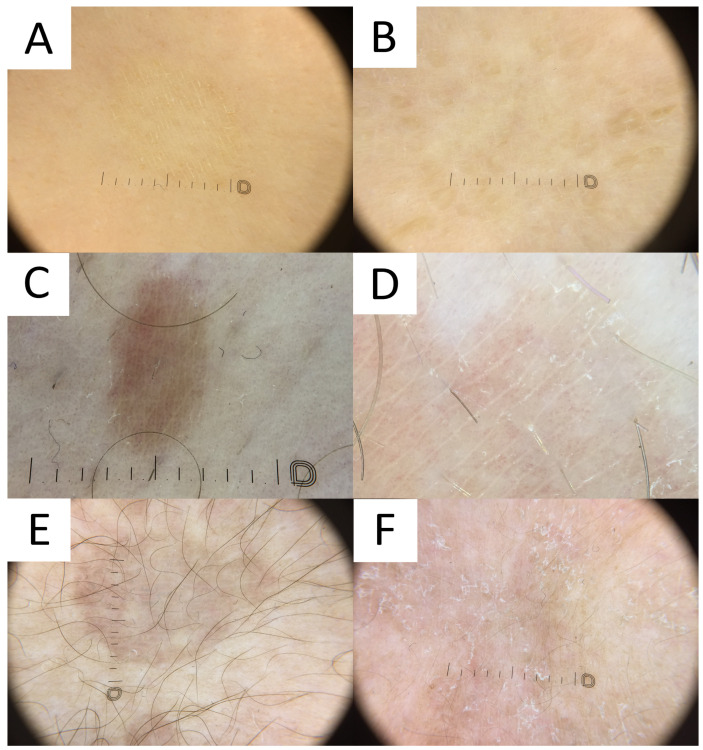
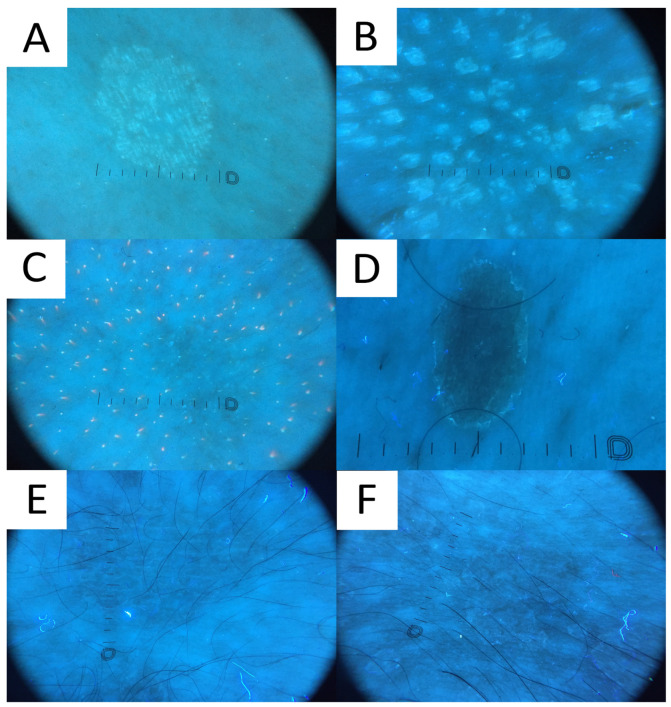
This narrative review presents a comprehensive overview of the diagnosis and management of pityriasis versicolor (PV), a common superficial fungal infection caused by the yeast Malassezia. PV is characterised by scaly hypopigmented or hyperpigmented patches, primarily affecting the upper trunk, neck, and upper arms. Regarding commensal interactions, Malassezia utilises nutrient sources without affecting the human host. In cases of pathogenicity, Malassezia can directly harm the host via virulence factors or toxins, or indirectly by triggering damaging host responses. The diagnosis typically relies on recognising characteristic clinical features. Due to the wide variability in its clinical presentation, recognising the differential diagnosis is critical. In this paper, we discuss the clinical differentials, with their dermatoscopic presentation, but also describe a range of helpful diagnostic techniques (microscopy, conventional and ultraviolet-induced fluorescence dermatoscopy, and confocal microscopy). Topical therapies are the primary treatment for PV, encompassing non-specific antifungal agents like sulphur with salicylic acid, selenium sulphide 2.5%, and zinc pyrithione. Additionally, specific topical antifungal medications with either fungicidal or fungistatic properties may also be incorporated into the topical treatment regimen, such as imidazoles, allylamines, and ciclopirox olamine. Systemic therapies might occasionally be used. Patient education and the promotion of good personal hygiene are pivotal to reduce the risk of recurrence. In recurrent cases, particularly during warmer and more humid periods, prolonged prophylaxis with topical agents should be considered.
Keywords: Malassezia; Pitryrosporum; confocal microscopy; dermatoscopy; fungal infections; imaging; microscopy; tinea versicolor; treatment; ultraviolet radiation; yeast.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Tinea versicolor: an updated review.Drugs Context. 2022 Nov 14;11:2022-9-2. doi: 10.7573/dic.2022-9-2. eCollection 2022. Drugs Context. 2022. PMID: 36452877 Free PMC article. Review.
-
Antifungal Treatment for Pityriasis Versicolor.J Fungi (Basel). 2015 Mar 12;1(1):13-29. doi: 10.3390/jof1010013. J Fungi (Basel). 2015. PMID: 29376896 Free PMC article. Review.
-
[Cutaneous Malassezia infections and Malassezia associated dermatoses: An update].Hautarzt. 2015 Jun;66(6):465-84; quiz 485-6. doi: 10.1007/s00105-015-3631-z. Hautarzt. 2015. PMID: 25968082 Review. German.
-
Management of seborrheic dermatitis and pityriasis versicolor.Am J Clin Dermatol. 2000 Mar-Apr;1(2):75-80. doi: 10.2165/00128071-200001020-00001. Am J Clin Dermatol. 2000. PMID: 11702314 Review.
-
Tinea versicolor in dark-skinned individuals.Int J Dermatol. 2014 Feb;53(2):137-41. doi: 10.1111/ijd.12345. Epub 2013 Dec 10. Int J Dermatol. 2014. PMID: 24320140 Review.
Cited by
-
When Pityriasis Versicolor wears a vitiligo mask: a puzzle in an immunocompromised patient.Oxf Med Case Reports. 2025 Jul 14;2025(7):omaf105. doi: 10.1093/omcr/omaf105. eCollection 2025 Jul. Oxf Med Case Reports. 2025. PMID: 40666061 Free PMC article.
-
Terra Firma-Forme Dermatosis: Clinical Insights, Dermoscopic and Ultraviolet-Induced Fluorescence Dermoscopy Findings-A Case Report and Literature Review.Case Rep Pediatr. 2025 Jul 16;2025:9349324. doi: 10.1155/crpe/9349324. eCollection 2025. Case Rep Pediatr. 2025. PMID: 40703495 Free PMC article.
-
The Human Mycobiome: Composition, Immune Interactions, and Impact on Disease.Int J Mol Sci. 2025 Jul 28;26(15):7281. doi: 10.3390/ijms26157281. Int J Mol Sci. 2025. PMID: 40806413 Free PMC article. Review.
-
Ultraviolet-induced Fluorescence Dermatoscopy Unmasks Dermatoscopically Inconspicuous Terra Firma-Forme Dermatosis and Pityriasis Versicolor.Dermatol Pract Concept. 2025 Apr 1;15(2):5211. doi: 10.5826/dpc.1502a5211. Dermatol Pract Concept. 2025. PMID: 40401850 Free PMC article. No abstract available.
-
A Double-Blind Randomised Clinical Trial of Terbinafine-Nanostructured Lipid Carriers: Should We Anticipate This Strategy for Effective Topical Treatment of Onychomycosis?Mycoses. 2025 Jun;68(6):e70076. doi: 10.1111/myc.70076. Mycoses. 2025. PMID: 40525269 Free PMC article. Clinical Trial.
References
Publication types
LinkOut - more resources
Full Text Sources
