

Susceptibility-based imaging aids accurate distinction of pediatric-onset MS from myelin oligodendrocyte glycoprotein antibody-associated disease
- PMID: 37897254
- PMCID: PMC10687802
- DOI: 10.1177/13524585231204414
Susceptibility-based imaging aids accurate distinction of pediatric-onset MS from myelin oligodendrocyte glycoprotein antibody-associated disease
Abstract
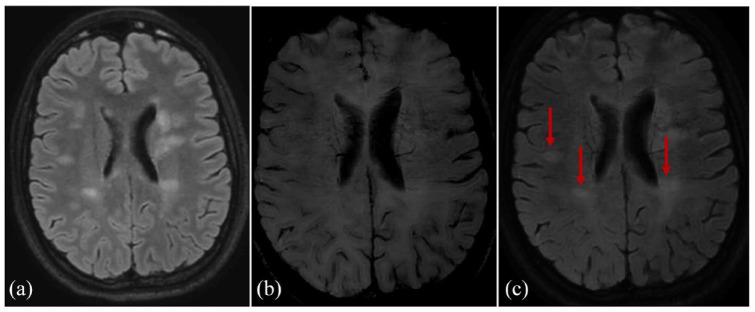
Background: Myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease (MOGAD) and pediatric-onset multiple sclerosis (POMS) share clinical and magnetic resonance imaging (MRI) features but differ in prognosis and management. Early POMS diagnosis is essential to avoid disability accumulation. Central vein sign (CVS), paramagnetic rim lesions (PRLs), and central core lesions (CCLs) are susceptibility-based imaging (SbI)-related signs understudied in pediatric populations that may help discerning POMS from MOGAD.
Methods: T2-FLAIR and SbI (three-dimensional echoplanar imaging (3D-EPI)/susceptibility-weighted imaging (SWI) or similar) were acquired on 1.5T/3T scanners. Two readers assessed CVS-positive rate (%CVS+), and their average score was used to build a receiver operator curve (ROC) assessing the ability to discriminate disease type. PRLs and CCLs were identified using a consensual approach.
Results: The %CVS+ distinguished 26 POMS cases (mean age 13.7 years, 63% females, median EDSS 1.5) from 14 MOGAD cases (10.8 years, 35% females, EDSS 1.0) with ROC = 1, p < 0.0001, (cutoff 41%). PRLs were only detectable in POMS participants (mean 2.1±2.3, range 1-10), discriminating the two conditions with a sensitivity of 69% and a specificity of 100%. CCLs were more sensitive (81%) but less specific (71.43%).
Conclusion: The %CVS+ and PRLs are highly specific markers of POMS. After proper validation on larger multicenter cohorts, consideration should be given to including such imaging markers for diagnosing POMS at disease onset.
Keywords: 3D-EPI; CVS; MOGAD; POMS; PRLs; SWI.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SS, NP, VAS, AA, HZ, JA, WAS, JC, JH, SSZ, PS, RGH, and EW have no disclosures relevant to this study.AV is supported by a Biogen Fellowship.
Figures






References
-
- Jurynczyk M, Geraldes R, Probert F, et al.. Distinct brain imaging characteristics of autoantibody-mediated CNS conditions and multiple sclerosis. Brain 2017; 140: 617–627. - PubMed
