

Intra-arterial peptide-receptor radionuclide therapy for neuro-endocrine tumour liver metastases: an in-patient randomised controlled trial (LUTIA)
- PMID: 37897617
- PMCID: PMC10881701
- DOI: 10.1007/s00259-023-06467-y
Intra-arterial peptide-receptor radionuclide therapy for neuro-endocrine tumour liver metastases: an in-patient randomised controlled trial (LUTIA)
Abstract
Purpose: Peptide receptor radionuclide therapy (PRRT) using [177Lu]Lu-DOTATATE has been shown to effectively prolong progression free survival in grade 1-2 gastroenteropancreatic neuroendocrine tumours (GEP-NET), but is less efficacious in patients with extensive liver metastases. The aim was to investigate whether tumour uptake in liver metastases can be enhanced by intra-arterial administration of [177Lu]Lu-DOTATATE into the hepatic artery, in order to improve tumour response without increasing toxicity.
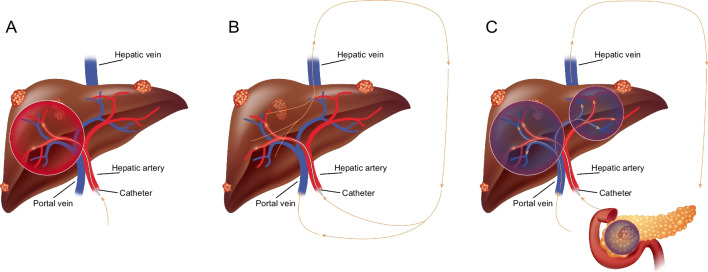
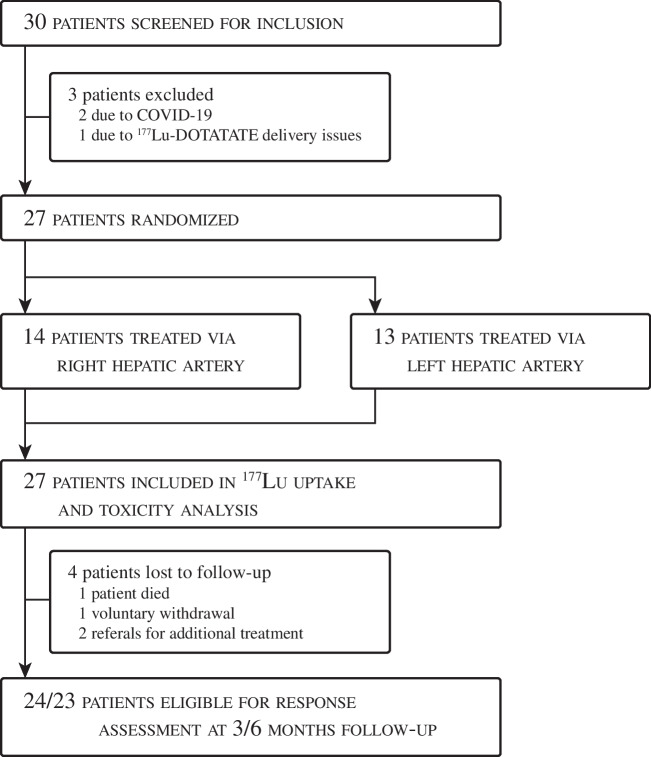
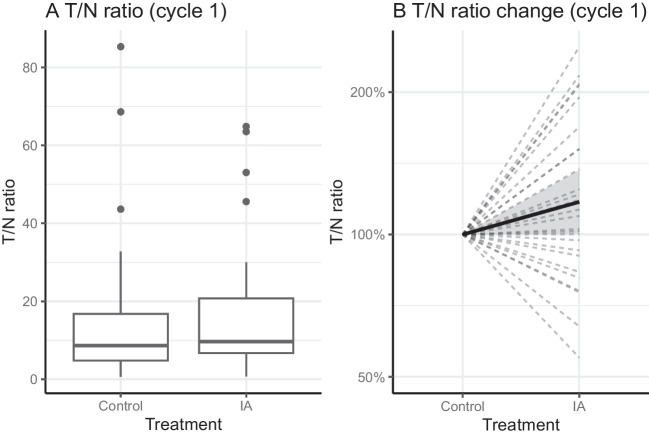
Methods: Twenty-seven patients with grade 1-2 GEP-NET, and bi-lobar liver metastases were randomized to receive intra-arterial PRRT in the left or right liver lobe for four consecutive cycles. The contralateral liver lobe and extrahepatic disease were treated via a "second-pass" effect and the contralateral lobe was used as the control lobe. Up to three metastases (> 3 cm) per liver lobe were identified as target lesions at baseline on contrast-enhanced CT. The primary endpoint was the tumour-to-non-tumour (T/N) uptake ratio on the 24 h post-treatment [177Lu]Lu-SPECT/CT after the first cycle. This was calculated for each target lesion in both lobes using the mean uptake. T/N ratios in both lobes were compared using paired-samples t-test.
Findings: After the first cycle, a non-significant difference in T/N uptake ratio was observed: T/NIA = 17·4 vs. T/Ncontrol = 16·2 (p = 0·299). The mean increase in T/N was 17% (1·17; 95% CI [1·00; 1·37]). Of all patients, 67% (18/27) showed any increase in T/N ratio after the first cycle.
Conclusion: Intra-arterial [177Lu]Lu-DOTATATE is safe, but does not lead to a clinically significant increase in tumour uptake.
Keywords: Efficacy; Intra-arterial; Neuroendocrine tumour; PRRT; Safety.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Niederle MB, Hackl M, Kaserer K, Niederle B. Gastroenteropancreatic neuroendocrine tumours: the current incidence and staging based on the WHO and European Neuroendocrine Tumour Society classification: an analysis based on prospectively collected parameters. Endocr Relat Cancer. 2010;17:909–918. doi: 10.1677/ERC-10-0152. - DOI - PubMed
-
- Lesén E, Granfeldt D, Berthon A, Dinet J, Houchard A, Myrenfors P, et al. Treatment patterns and survival among patients with metastatic gastroenteropancreatic neuroendocrine tumours in Sweden-a population-based register-linkage and medical chart review study. J Cancer. 2019;10:6876–6887. doi: 10.7150/jca.32381. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
