

Complementary structural and functional abnormalities to localise epileptogenic tissue
- PMID: 37898096
- PMCID: PMC10630610
- DOI: 10.1016/j.ebiom.2023.104848
Complementary structural and functional abnormalities to localise epileptogenic tissue
Abstract
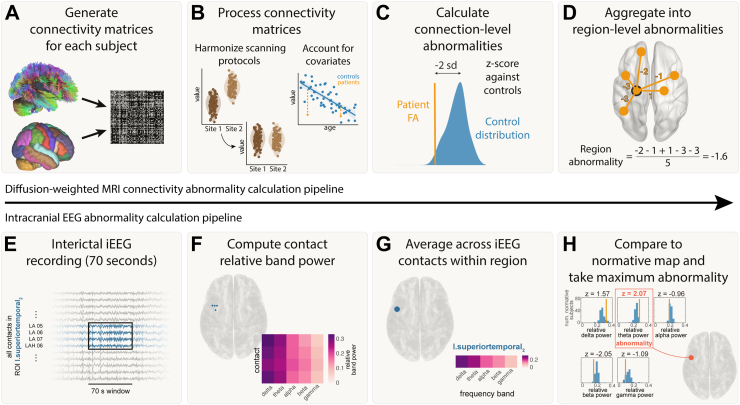
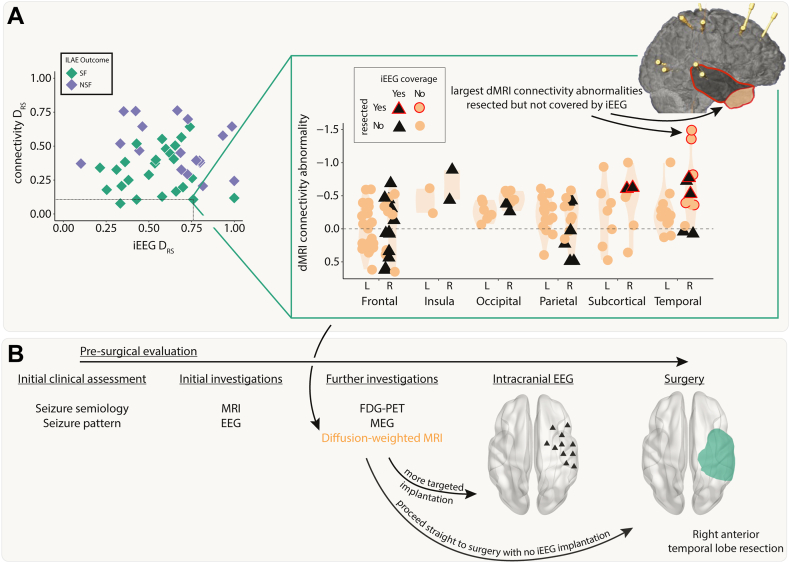
Background: When investigating suitability for epilepsy surgery, people with drug-refractory focal epilepsy may have intracranial EEG (iEEG) electrodes implanted to localise seizure onset. Diffusion-weighted magnetic resonance imaging (dMRI) may be acquired to identify key white matter tracts for surgical avoidance. Here, we investigate whether structural connectivity abnormalities, inferred from dMRI, may be used in conjunction with functional iEEG abnormalities to aid localisation of the epileptogenic zone (EZ), improving surgical outcomes in epilepsy.
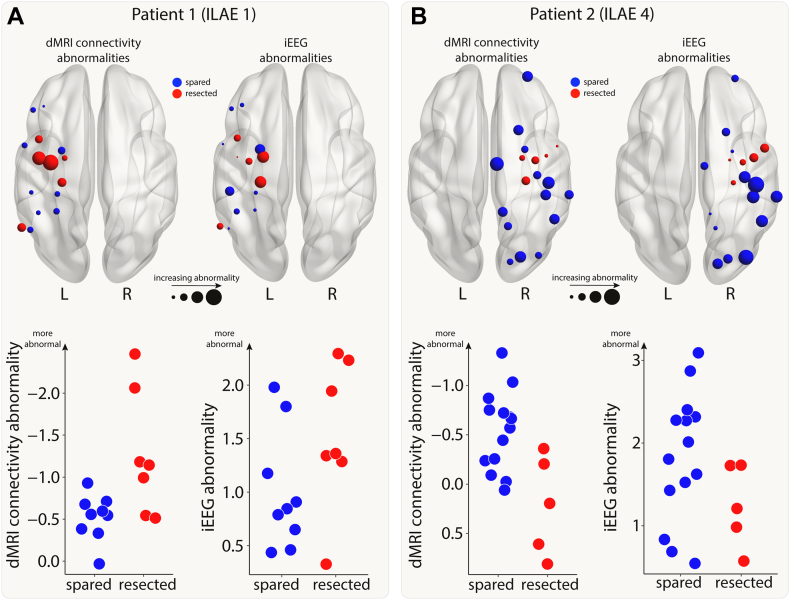
Methods: We retrospectively investigated data from 43 patients (42% female) with epilepsy who had surgery following iEEG. Twenty-five patients (58%) were free from disabling seizures (ILAE 1 or 2) at one year. Interictal iEEG functional, and dMRI structural connectivity abnormalities were quantified by comparison to a normative map and healthy controls. We explored whether the resection of maximal abnormalities related to improved surgical outcomes, in both modalities individually and concurrently. Additionally, we suggest how connectivity abnormalities may inform the placement of iEEG electrodes pre-surgically using a patient case study.
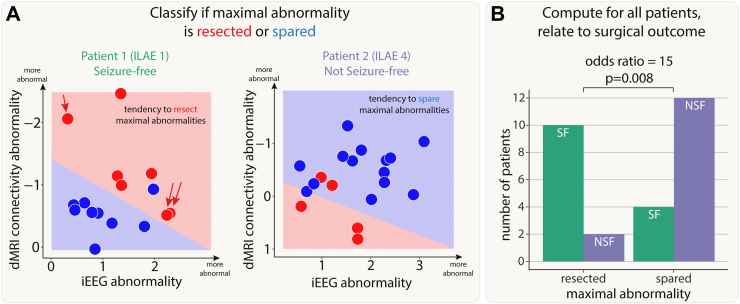
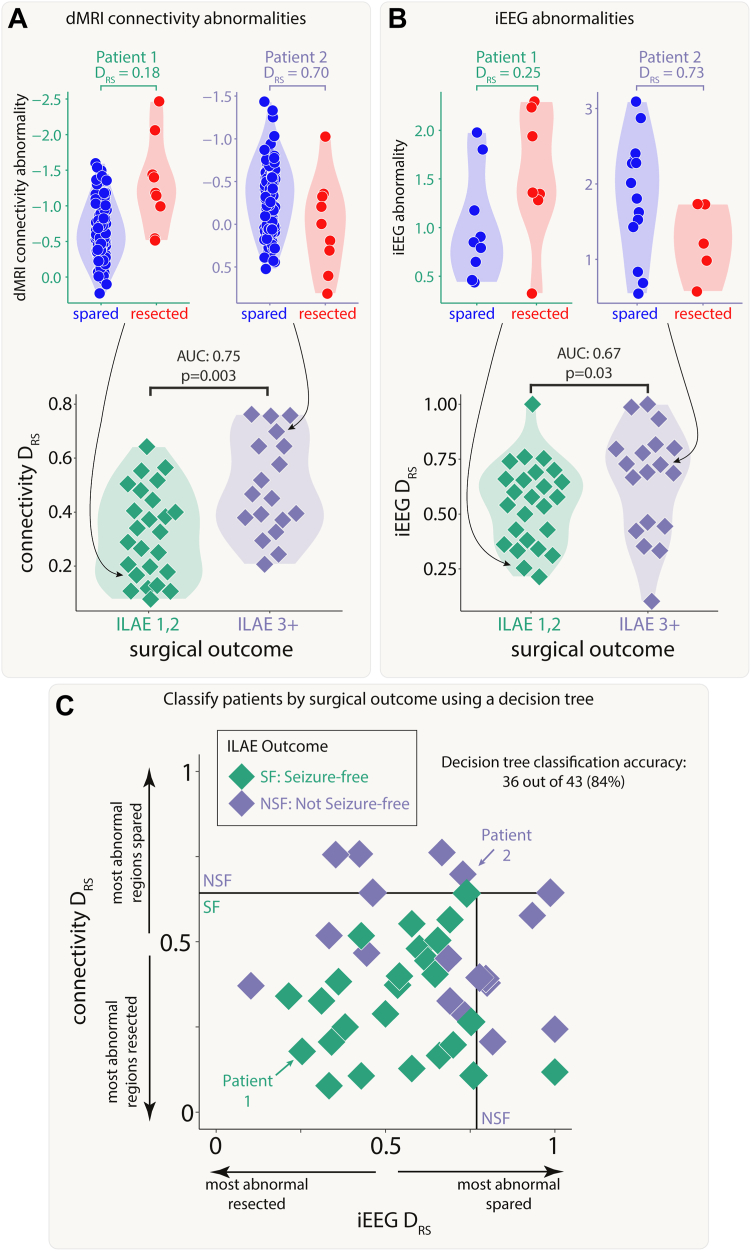
Findings: Seizure freedom was 15 times more likely in patients with resection of maximal connectivity and iEEG abnormalities (p = 0.008). Both modalities separately distinguished patient surgical outcome groups and when used simultaneously, a decision tree correctly separated 36 of 43 (84%) patients.
Interpretation: Our results suggest that both connectivity and iEEG abnormalities may localise epileptogenic tissue, and that these two modalities may provide complementary information in pre-surgical evaluations.
Funding: This research was funded by UKRI, CDT in Cloud Computing for Big Data, NIH, MRC, Wellcome Trust and Epilepsy Research UK.
Keywords: Diffusion-weighted MRI; Epilepsy; Intracranial EEG; Machine learning; Multi-modal analysis; Surgical prediction.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests J.H. received support for attending meetings and/or travel from the Centre for Doctoral Training in Cloud Computing for Big Data (EP/L015358/1). R.T. received consulting fees from Angelini, Jazz. RT received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Angelini, Bial, Biocodex, Eisai, Jazz, LivaNova, Neuraxpharm, Sanofi, Takeda, UCB Pharma and Zogenix. RT Participated on a Data Safety Monitoring Board or Advisory Board for Angelini, LivaNova, Sanofi, UCB. RT has a Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as Treasurer British Branch ILAE; Trustee of Epilepsy Research UK. MW received royalties or licenses from Vitaflo. MW received consulting fees from Ambrosetti and EpilepsyGtx. MW received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Angelini and UCB Pharma. MW has the following patents (planned, issued or pending) WO2018229254A1 EP3116508A1 US10301263B2 WO2023152318A1 CA3058047A1 EP2642990B1 CA3064329A1. MW has a leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid at Epilepsy Research UK, and the International League against Epilepsy. PT received funding for a PhD studentship from Epilepsy Research UK.
Figures
Update of
-
Complementary structural and functional abnormalities to localise epileptogenic tissue.ArXiv [Preprint]. 2023 Oct 24:arXiv:2304.03192v3. ArXiv. 2023. Update in: EBioMedicine. 2023 Nov;97:104848. doi: 10.1016/j.ebiom.2023.104848. PMID: 37064531 Free PMC article. Updated. Preprint.
