

Associations of dietary patterns with kidney cancer risk, kidney cancer-specific mortality and all-cause mortality among postmenopausal women
- PMID: 37898720
- PMCID: PMC10703863
- DOI: 10.1038/s41416-023-02469-7
Associations of dietary patterns with kidney cancer risk, kidney cancer-specific mortality and all-cause mortality among postmenopausal women
Abstract
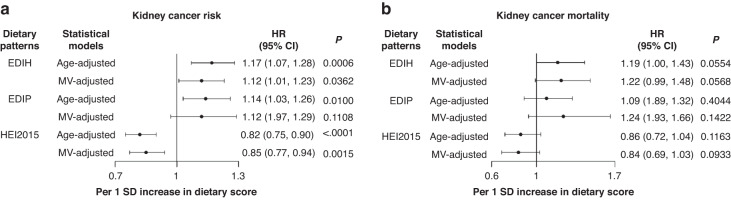
Background: The empirical dietary index for hyperinsulinemia (EDIH) and empirical dietary inflammatory pattern (EDIP) are novel measures of dietary quality associated with insulin hypersecretion or chronic inflammation, respectively, whereas the Healthy Eating Index (HEI-2015) measures adherence to the Dietary Guidelines for Americans (DGA). We evaluated associations of EDIH, EDIP and HEI-2015 on the risk of both kidney cancer development and mortality.
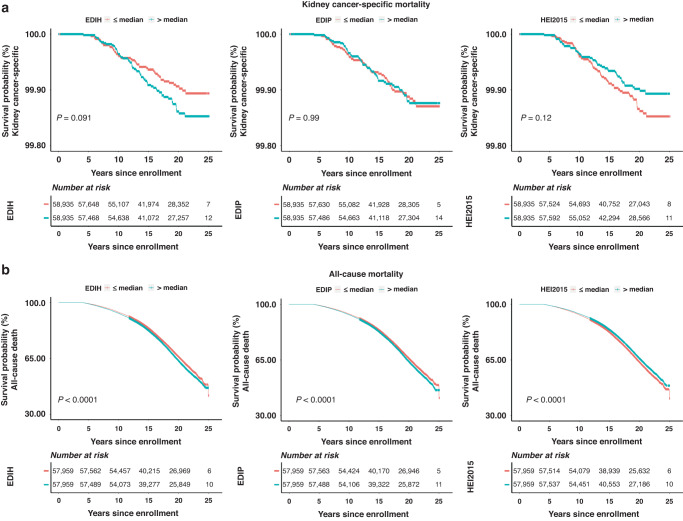
Methods: We calculated the dietary scores from baseline food frequency questionnaires among 115,830 participants aged 50-79 years in the Women's Health Initiative. Multivariable-adjusted Cox regression was used to estimate hazard ratios (HR) and 95% confidence intervals (95%CI) for kidney cancer risk, kidney cancer-specific mortality and all-cause mortality, per 1-standard deviation increment in dietary pattern scores.
Results: Higher EDIH was associated with greater risk of kidney cancer development [HR, 1.12; 95%CI, (1.01,1.23)], kidney cancer-specific death [1.22(0.99,1.48)], and all-cause mortality, [1.05(1.02,1.08)]. Higher HEI-2015 was associated with lower risk of kidney cancer development, [0.85(0.77, 0.94)], kidney cancer-specific death, [0.84(0.69,1.03)] and all-cause mortality, [0.97(0.95,1.00)]. However, EDIP was not significantly associated with outcomes. Associations did not differ by BMI categories.
Conclusions: Low-insulinemic dietary patterns and higher quality diets, are worthy of testing in dietary pattern intervention trials for kidney cancer prevention and improved survivorship.
© 2023. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Collaboration GBoDC. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019;5:1749–68. doi: 10.1001/jamaoncol.2019.2996. - DOI - PMC - PubMed
-
- Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (2018); 392: 1736-88; e-pub ahead of print 2018/11/30; 10.1016/s0140-6736(18)32203-7. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
