

Geospatial patterns of progress towards UNAIDS '95-95-95' targets and community vulnerability in Zambia: insights from population-based HIV impact assessments
- PMID: 37899088
- PMCID: PMC10619088
- DOI: 10.1136/bmjgh-2023-012629
Geospatial patterns of progress towards UNAIDS '95-95-95' targets and community vulnerability in Zambia: insights from population-based HIV impact assessments
Abstract
Introduction: In sub-Saharan Africa, HIV/AIDS remains a leading cause of death. The UNAIDS established the '95-95-95' targets to improve HIV care continuum outcomes. Using geospatial data from the Zambia Population-based HIV Impact Assessment (ZAMPHIA), this study aims to investigate geospatial patterns in the '95-95-95' indicators and individual-level determinants that impede HIV care continuum in vulnerable communities, providing insights into the factors associated with gaps.
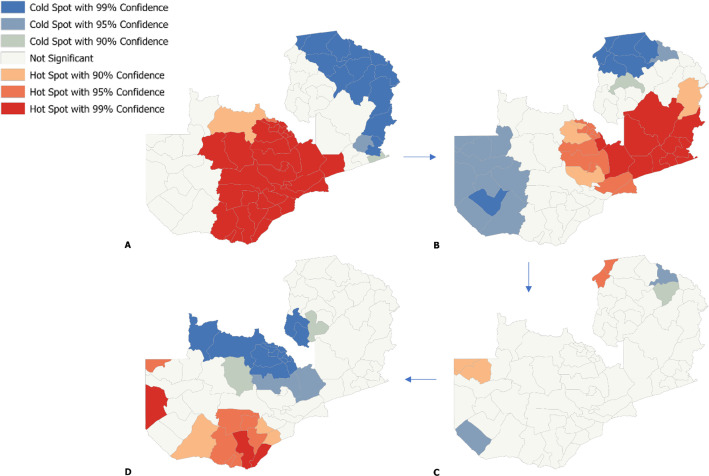
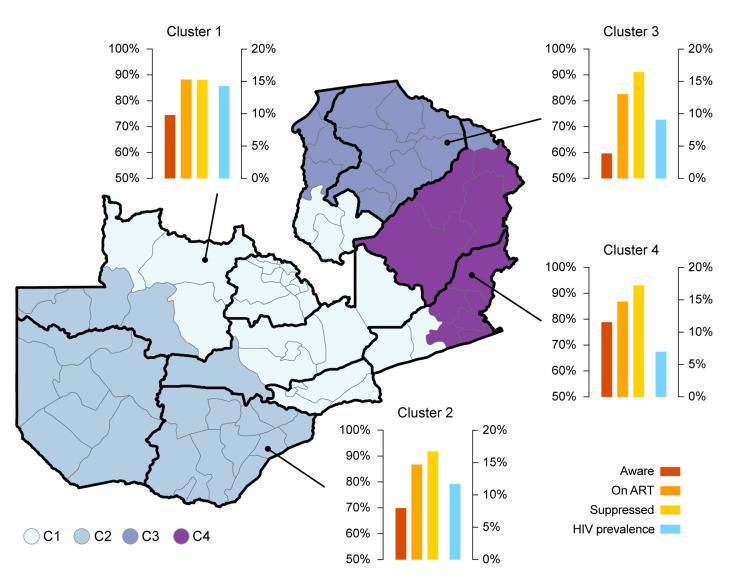
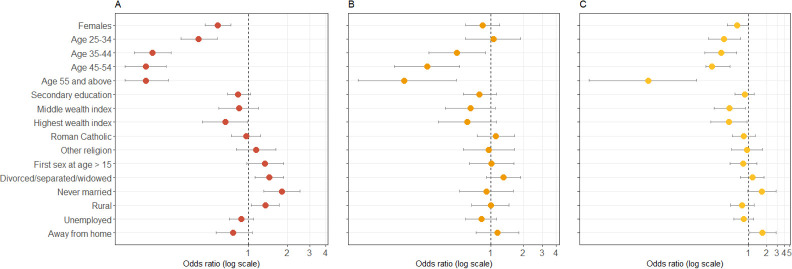
Methods: This study used data from the 2016 ZAMPHIA to investigate the geospatial distribution and individual-level determinants of engagement across the HIV care continuum in Zambia. Gaussian kernel interpolation and optimised hotspot analysis were used to identify geospatial patterns in the HIV care continuum, while geospatial k-means clustering was used to partition areas into clusters. The study also assessed healthcare availability, access and social determinants of healthcare utilisation. Multiple logistic regression models were used to examine the association between selected sociodemographic and behavioural covariates and the three main outcomes of study.
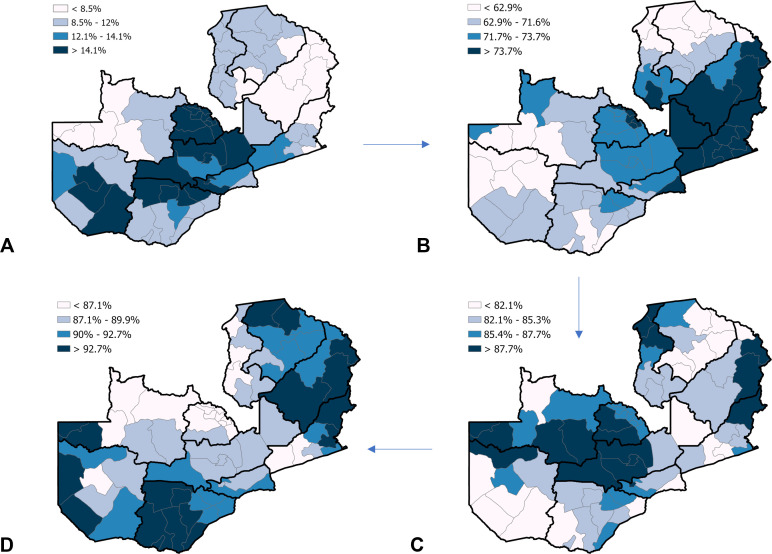
Results: Varied progress towards the '95-95-95' targets were observed in different regions of Zambia. Each '95' displayed a unique geographical pattern, independent of HIV prevalence, resulting in four distinct geographical clusters. Factors associated with gaps in the '95s' include younger age, male sex, and low wealth, with younger individuals having higher odds of not being on antiretroviral therapy and having detectable viral loads.
Conclusions: Our study revealed significant spatial heterogeneity in the HIV care continuum in Zambia, with different regions exhibiting unique geographical patterns and levels of performance in the '95-95-95' targets, highlighting the need for geospatial tailored interventions to address the specific needs of different subnational regions. These findings underscore the importance of addressing differential regional gaps in HIV diagnosis, enhancing community-level factors and developing innovative strategies to improve local HIV care continuum outcomes.
Keywords: AIDS; Epidemiology; Geographic information systems; HIV.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Update of
-
Geospatial Patterns of Progress towards UNAIDS "95-95-95" Targets and Community Vulnerability in Zambia.medRxiv [Preprint]. 2023 Apr 26:2023.04.24.23289044. doi: 10.1101/2023.04.24.23289044. medRxiv. 2023. Update in: BMJ Glob Health. 2023 Oct;8(10):e012629. doi: 10.1136/bmjgh-2023-012629. PMID: 37163012 Free PMC article. Updated. Preprint.
Similar articles
-
Assessing regional variations and sociodemographic barriers in the progress toward UNAIDS 95-95-95 targets in Zimbabwe.Commun Med (Lond). 2025 Apr 9;5(1):106. doi: 10.1038/s43856-025-00824-8. Commun Med (Lond). 2025. PMID: 40204867 Free PMC article.
-
Progress Towards UNAIDS's 95-95-95 Targets in Zimbabwe: Sociodemographic Constraints and Geospatial Heterogeneity.medRxiv [Preprint]. 2023 Jul 28:2023.07.26.23293207. doi: 10.1101/2023.07.26.23293207. medRxiv. 2023. PMID: 37546877 Free PMC article. Preprint.
-
Moving beyond hotspots of HIV prevalence to geospatial hotspots of UNAIDS 95-95-95 targets in sub-Saharan Africa.Lancet HIV. 2024 Jul;11(7):e479-e488. doi: 10.1016/S2352-3018(24)00102-4. Epub 2024 Jun 6. Lancet HIV. 2024. PMID: 38852597 Free PMC article. Review.
-
Geospatial Patterns of Progress towards UNAIDS "95-95-95" Targets and Community Vulnerability in Zambia.medRxiv [Preprint]. 2023 Apr 26:2023.04.24.23289044. doi: 10.1101/2023.04.24.23289044. medRxiv. 2023. Update in: BMJ Glob Health. 2023 Oct;8(10):e012629. doi: 10.1136/bmjgh-2023-012629. PMID: 37163012 Free PMC article. Updated. Preprint.
-
Men missing from the HIV care continuum in sub-Saharan Africa: a meta-analysis and meta-synthesis.J Int AIDS Soc. 2022 Mar;25(3):e25889. doi: 10.1002/jia2.25889. J Int AIDS Soc. 2022. PMID: 35324089 Free PMC article. Review.
Cited by
-
Assessing regional variations and sociodemographic barriers in the progress toward UNAIDS 95-95-95 targets in Zimbabwe.Commun Med (Lond). 2025 Apr 9;5(1):106. doi: 10.1038/s43856-025-00824-8. Commun Med (Lond). 2025. PMID: 40204867 Free PMC article.
-
Trend of HIV Prevalence in Antenatal Women in a Tertiary Care Hospital in the Western Region of India.Cureus. 2024 Mar 28;16(3):e57125. doi: 10.7759/cureus.57125. eCollection 2024 Mar. Cureus. 2024. PMID: 38567207 Free PMC article.
-
Progress Towards UNAIDS's 95-95-95 Targets in Zimbabwe: Sociodemographic Constraints and Geospatial Heterogeneity.medRxiv [Preprint]. 2023 Jul 28:2023.07.26.23293207. doi: 10.1101/2023.07.26.23293207. medRxiv. 2023. PMID: 37546877 Free PMC article. Preprint.
-
Moving beyond hotspots of HIV prevalence to geospatial hotspots of UNAIDS 95-95-95 targets in sub-Saharan Africa.Lancet HIV. 2024 Jul;11(7):e479-e488. doi: 10.1016/S2352-3018(24)00102-4. Epub 2024 Jun 6. Lancet HIV. 2024. PMID: 38852597 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical