

Increasing trends of overweight and obesity in treatment-naive people living with HIV in Shenzhen from 2014 to 2020: an emerging health concern
- PMID: 37900013
- PMCID: PMC10602863
- DOI: 10.3389/fpubh.2023.1186838
Increasing trends of overweight and obesity in treatment-naive people living with HIV in Shenzhen from 2014 to 2020: an emerging health concern
Abstract
Background: With the early initiation of antiretroviral therapy (ART) in China, the demographics of treatment-naïve people living with HIV (PLWH) are moving closer to those of the general population, which is characterized by a gradual increase in metabolic indicators. However, the epidemic trends of overweight and obesity over the past decade in treatment-naïve PLWH ready to initiate ART have not yet been investigated.
Methods: A cross-sectional study was conducted, including 12,135 consecutive treatment-naïve PLWH ready to initiate ART in Shenzhen, using data retrieved from the China National Free Antiretroviral Treatment Program database from 2014 to 2020. The chi-square test was used to examine the trends of overweight and obesity between age groups, and multivariate logistic regression was used to identify the association of overweight and obesity with hyperglycemia and dyslipidemia.
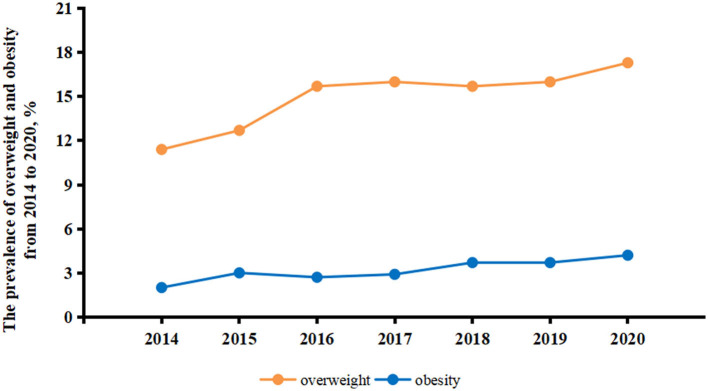
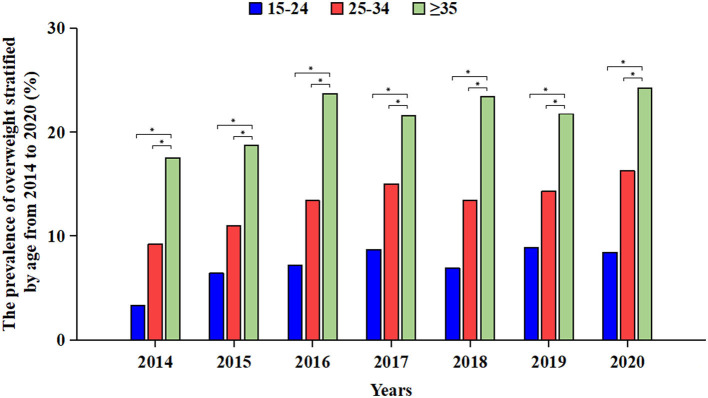
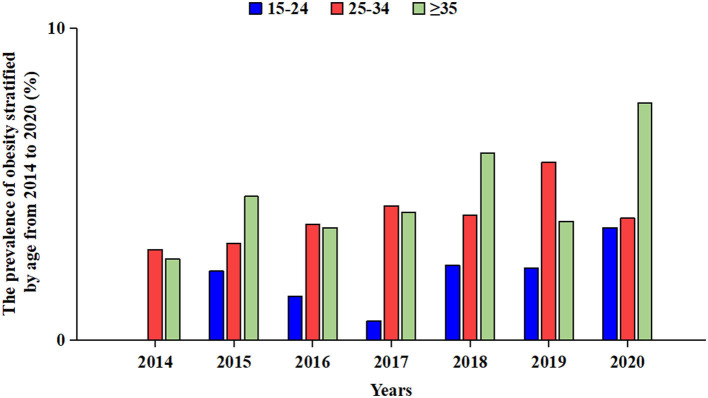
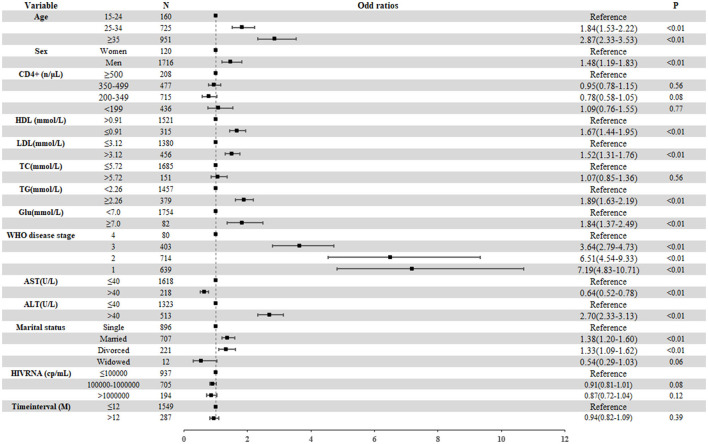
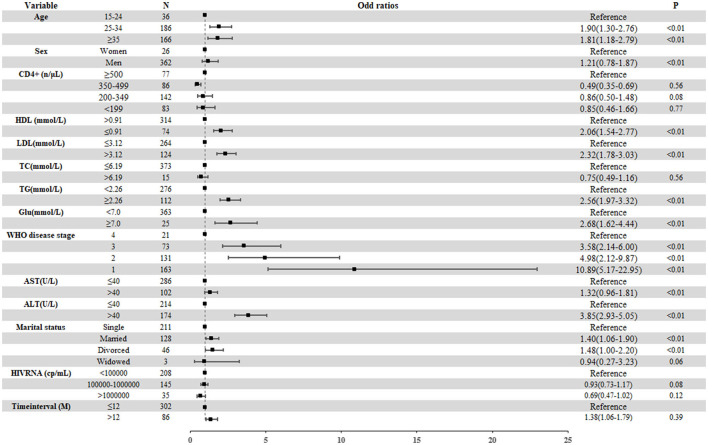
Results: During the 7-year study period, 12,135 treatment-naïve PLWH ready to initiate ART were included, among whom 1,837 (15.1%) were overweight and 388 (3.2%) were obese. The prevalence of overweight rose from 11.4 to 17.3% (Z = -4.58, P for trend <0.01) and that of obesity from 2.0% to 4.2% (Z = -6.45, P for trend <0.01) from 2014 to 2020. The annual prevalence of overweight was the highest in the age group of participants >35 years compared to prevalence in other age groups during the period 2014-2020. Compared with those who were not overweight or obese, PLWH who were overweight or obese were more likely to have hyperglycemia (aOR 1.84, 95% CI: 1.37-2.49 for overweight; aOR 2.68, 95% CI: 1.62-4.44 for obesity), higher ALT level (aOR 2.70, 95% CI: 2.33-3.13 for overweight; aOR 3.85, 95% CI: 2.93-5.05 for obesity), higher TG levels (aOR 1.89, 95% CI 1.63-2.19 for overweight; aOR 2.56, 95% CI 1.97-3.32 for obesity), and lower HDL levels (aOR 1.67, 95% CI 1.44-1.95 for overweight; aOR 2.06, 95% CI 1.54-2.77 for obesity).
Conclusion: The prevalence of overweight and obesity in treatment-naive PLWH increased steadily from 2014 to 2020 in Shenzhen. Overweight and obese in treatment-naive PLWH ready to initiate ART were associated with dyslipidemia and hyperglycemia. Public health authorities should take proactive steps to address these issues by implementing targeted screening, intervention programs including lifestyle modifications, and integrated healthcare services.
Keywords: consecutive cross-sectional study; obesity; overweight; people living with HIV; treatment-naïve.
Copyright © 2023 Li, Sun, He, Zhou, Xu, Zhao, Hu, Wang, Lu and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Evolution of blood lipids and risk factors of dyslipidemia among people living with human immunodeficiency virus who had received first-line antiretroviral regimens for 3 years in Shenzhen.Chin Med J (Engl). 2020 Dec 5;133(23):2808-2815. doi: 10.1097/CM9.0000000000001245. Chin Med J (Engl). 2020. PMID: 33273329 Free PMC article.
-
High prevalence of being Overweight and Obese HIV-infected persons, before and after 24 months on early ART in the ANRS 12136 Temprano Trial.AIDS Res Ther. 2016 Feb 25;13:12. doi: 10.1186/s12981-016-0094-y. eCollection 2016. AIDS Res Ther. 2016. PMID: 26925155 Free PMC article. Clinical Trial.
-
Metabolic syndrome among treatment-naïve people living with and without HIV in Zambia and Zimbabwe: a cross-sectional analysis.J Int AIDS Soc. 2022 Dec;25(12):e26047. doi: 10.1002/jia2.26047. J Int AIDS Soc. 2022. PMID: 36522287 Free PMC article.
-
Metabolic Profile of People Living with HIV in a Treatment Hub in Manila, Philippines: A Pre- and Post-Antiretroviral Analysis.J ASEAN Fed Endocr Soc. 2022;37(1):53-61. doi: 10.15605/jafes.037.01.17. Epub 2022 Feb 18. J ASEAN Fed Endocr Soc. 2022. PMID: 35800599 Free PMC article. Review.
-
Diabetes in People Living with HIV.2023 Nov 1. In: Feingold KR, Ahmed SF, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–. 2023 Nov 1. In: Feingold KR, Ahmed SF, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–. PMID: 31479220 Free Books & Documents. Review.
Cited by
-
Abdominal adiposity is negatively associated with physical function among people with HIV.AIDS. 2025 Jul 1;39(8):986-994. doi: 10.1097/QAD.0000000000004168. Epub 2025 Mar 4. AIDS. 2025. PMID: 40053478
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous