

Pancreatic arteriovenous malformation treated with transcatheter arterial embolization: Two case reports and review of literature
- PMID: 37901023
- PMCID: PMC10600833
- DOI: 10.12998/wjcc.v11.i28.6920
Pancreatic arteriovenous malformation treated with transcatheter arterial embolization: Two case reports and review of literature
Abstract
Background: Various treatment methods are available for the treatment of pancreatic arteriovenous malformation (P-AVM); however, there are no established treatment options for asymptomatic P-AVM.
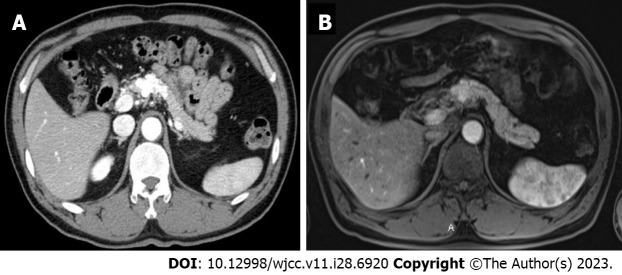
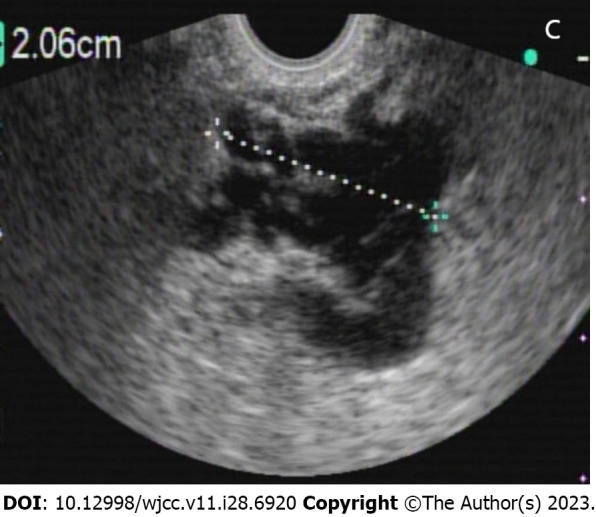
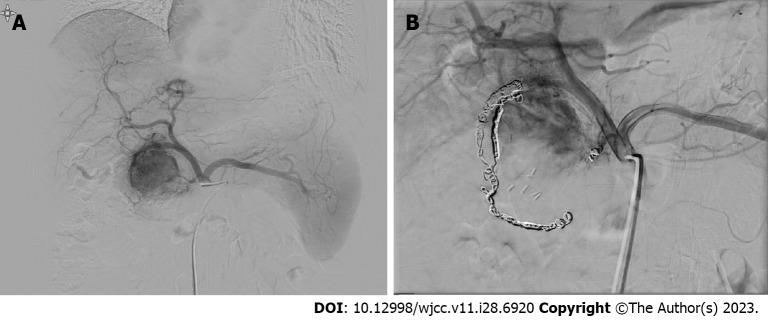
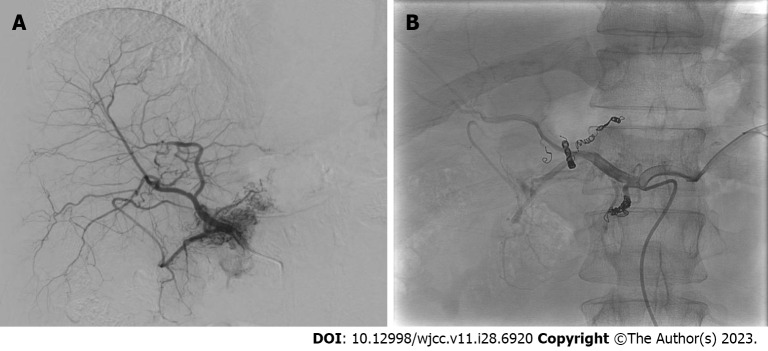
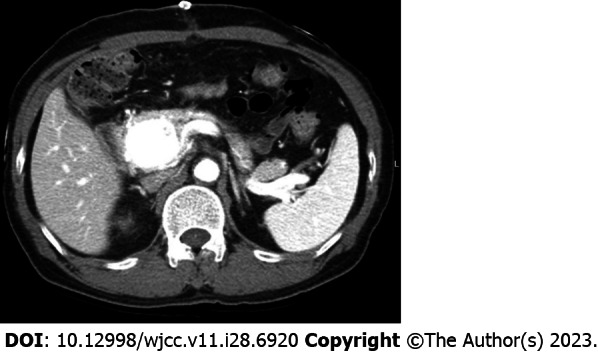
Case summary: A 47-year-old and a 50-year-old male patients sought treatment for P-AVM in the pancreas, which was incidentally detected during routine abdominal computed tomography and magnetic resonance imaging conducted as part of a health check-up. They underwent transcatheter arterial embolization (TAE), and over the course of a 9-year follow-up period, the AVM did not worsen and was asymptomatic.
Conclusion: TAE can be considered as an alternative treatment option for P-AVM in selective cases where patients are asymptomatic or have a high surgical risk.
Keywords: Angiography; Asymptomatic; Case report; Pancreatic arteriovenous malformation; Surgical treatment; Transcatheter arterial embolization.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no competing interests.
Figures


Similar articles
-
Embolization of pancreatic arteriovenous malformation: A case report.World J Clin Cases. 2020 Apr 26;8(8):1471-1476. doi: 10.12998/wjcc.v8.i8.1471. World J Clin Cases. 2020. PMID: 32368539 Free PMC article.
-
A successful case of transcatheter arterial embolization with n-butyl-2-cyanoacrylate for pancreatic arteriovenous malformation.Intern Med. 2014;53(23):2683-7. doi: 10.2169/internalmedicine.53.3327. Epub 2014 Dec 1. Intern Med. 2014. PMID: 25447650 Review.
-
Pancreatic arteriovenous malformation involving the duodenum embolized with ethylene-vinyl alcohol copolymer (Onyx).Cardiovasc Intervent Radiol. 2012 Aug;35(4):958-62. doi: 10.1007/s00270-011-0272-1. Epub 2011 Sep 28. Cardiovasc Intervent Radiol. 2012. PMID: 21953209
-
Surgical resection of arteriovenous malformation of the pancreatic head with acute pancreatitis: a case report.J Surg Case Rep. 2022 Sep 28;2022(9):rjac427. doi: 10.1093/jscr/rjac427. eCollection 2022 Sep. J Surg Case Rep. 2022. PMID: 36196137 Free PMC article.
-
Management of pancreatic arteriovenous malformation: Case report and literature review.Medicine (Baltimore). 2021 Dec 23;100(51):e27983. doi: 10.1097/MD.0000000000027983. Medicine (Baltimore). 2021. PMID: 34941037 Free PMC article. Review.
References
-
- Halpern M, Turner AF, Citron BP. Hereditary hemorrhagic telangiectasia. An angiographic study of abdominal visceral angiodysplasias associated with gastrointestinal hemorrhage. Radiology. 1968;90:1143–1149. - PubMed
-
- Sharma M, Bedi MM, Mahesh S, Gandhi MD, Antony R, Mukkada RJ, Lekha V, Ramesh H. Arteriovenous malformation of the pancreatic head--difficulties in diagnosis and treatment. Indian J Gastroenterol. 2011;30:46–48. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
