

World Heart Federation Consensus on Transthyretin Amyloidosis Cardiomyopathy (ATTR-CM)
- PMID: 37901600
- PMCID: PMC10607607
- DOI: 10.5334/gh.1262
World Heart Federation Consensus on Transthyretin Amyloidosis Cardiomyopathy (ATTR-CM)
Abstract
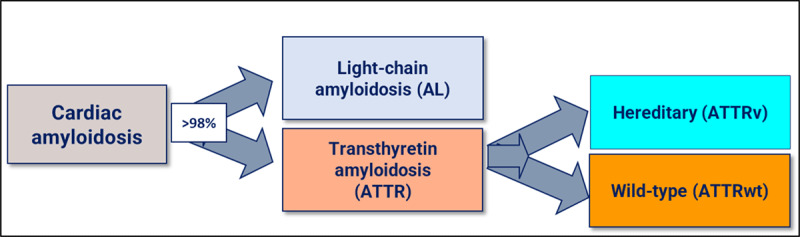
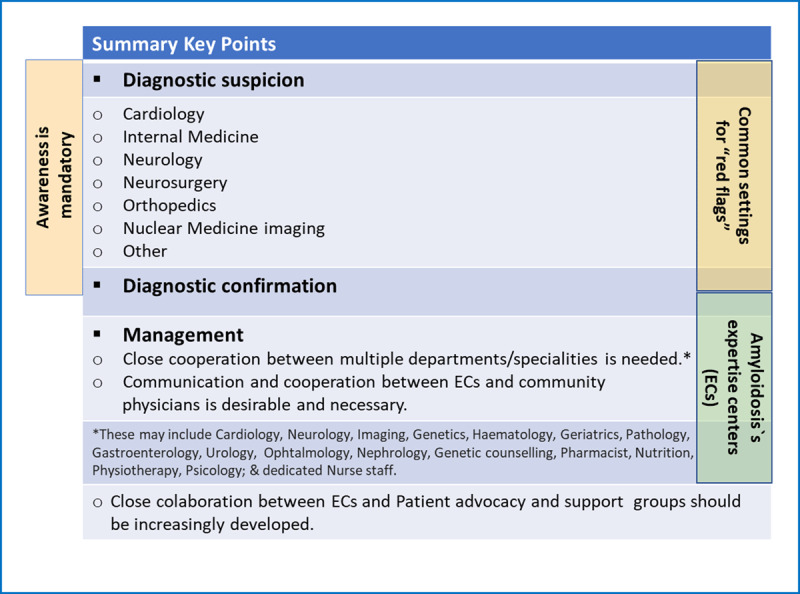
Transthyretin amyloid cardiomyopathy (ATTR-CM) is a progressive and fatal condition that requires early diagnosis, management, and specific treatment. The availability of new disease-modifying therapies has made successful treatment a reality. Transthyretin amyloid cardiomyopathy can be either age-related (wild-type form) or caused by mutations in the TTR gene (genetic, hereditary forms). It is a systemic disease, and while the genetic forms may exhibit a variety of symptoms, a predominant cardiac phenotype is often present. This document aims to provide an overview of ATTR-CM amyloidosis focusing on cardiac involvement, which is the most critical factor for prognosis. It will discuss the available tools for early diagnosis and patient management, given that specific treatments are more effective in the early stages of the disease, and will highlight the importance of a multidisciplinary approach and of specialized amyloidosis centres. To accomplish these goals, the World Heart Federation assembled a panel of 18 expert clinicians specialized in TTR amyloidosis from 13 countries, along with a representative from the Amyloidosis Alliance, a patient advocacy group. This document is based on a review of published literature, expert opinions, registries data, patients' perspectives, treatment options, and ongoing developments, as well as the progress made possible via the existence of centres of excellence. From the patients' perspective, increasing disease awareness is crucial to achieving an early and accurate diagnosis. Patients also seek to receive care at specialized amyloidosis centres and be fully informed about their treatment and prognosis.
Keywords: Amyloidosis; Heart Failure; Transthyretin amyloid cardiomyopathy (ATTR-CM); diagnosis; patients’ perspective; treatment.
Copyright: © 2023 The Author(s).
Conflict of interest statement
D.B. declares speaking fees from Alnylam Pharmaceuticals, AstraZeneca, Bayer, Bial, Merck Serono, Novartis, Pfizer and Vifor Pharma, consulting fees from Alnylam Pharmaceuticals, AstraZeneca, Bayer, Bial, Boehringer Ingelheim, Novartis, Pfizer and Vifor Pharma, and research/educational support to her institution from Alnylam Pharmaceuticals, Novartis, and NovoNordisk. D.P.A. declares honoraria from Pfizer for lectures. N.B. declares speaking fees and research grants from Pfizer. N.B. declares medical consulting fees from Pfizer. T.D. declares honoraria or educational grants and consultancies from Alnylam, Akcea, Ionis, Pfizer, Novonordisc, GSK, Neurimmune and AstraZeneca. S.D. declares research grants from Pfizer, Attralus, GE Healthcare, Phillips and honoraria from Novo Nordisk and Astra Zeneca. P.G.P. reports speaking fees from Alnylam Pharmaceuticals, AstraZeneca, Bridgebio, Ionis Pharmaceuticals, NovoNordisk, and Pfizer; consulting fees from Alexion, Alnylam Pharmaceuticals, AstraZeneca, ATTRalus, Bridgebio, General Electric, Intellia, Neurimmune, NovoNordisk, and Pfizer. J.D.G declares consulting fee from Alnylam, Intellia, Ionis, AstraZeneca, ATTRalus, Eidos. J.G. declares honoraria consultancy from Pfizer; L.B. declares honoraria for consultancy and/or participation in speakers’ bureau from Alnylam, Pfizer, SOBI, Astra Zeneca, Novo Nordisk and BridgeBio. M.U. declares grants, personal fees and non-financial support from Pfizer and Alnylam Pharmaceuticals, personal fees from Janssen Pharmaceutical K.K., outside the submitted work. The other authors declare no conflict of interests.
Figures


Comment in
-
Standardising Care and Treatment of Transthyretin Amyloid Cardiomyopathy.Glob Heart. 2023 Nov 20;18(1):63. doi: 10.5334/gh.1275. eCollection 2023. Glob Heart. 2023. PMID: 38028963 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
