

Effects of Steady Glucose Concentration Peritoneal Dialysis on Ultrafiltration Volume and Sodium Removal: A Pilot Crossover Trial
- PMID: 37902732
- PMCID: PMC10861104
- DOI: 10.2215/CJN.0000000000000342
Effects of Steady Glucose Concentration Peritoneal Dialysis on Ultrafiltration Volume and Sodium Removal: A Pilot Crossover Trial
Abstract
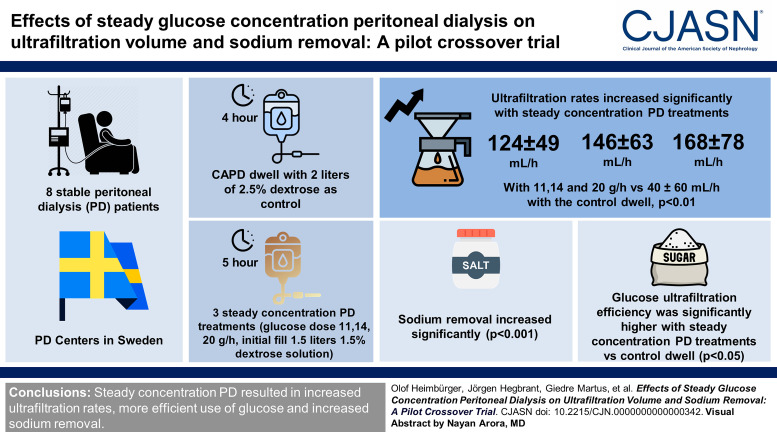
Background: Volume overload is common in patients treated with peritoneal dialysis (PD) and is associated with poor clinical outcome. Steady concentration PD is where a continuous glucose infusion maintains the intraperitoneal glucose concentration and as a result provides continuous ultrafiltration throughout the dwell. The primary objective of this study was to investigate the ultrafiltration rate and glucose ultrafiltration efficiency for steady concentration PD in comparison with a standard continuous ambulatory PD (CAPD) dwell, using the novel Carry Life UF device.
Methods: Eight stable patients treated with PD (six fast and two fast average transporters) were investigated four times: a standard 4-hour CAPD dwell with 2 L of 2.5% dextrose solution as control and three 5-hour steady concentration PD treatments (glucose dose 11, 14, 20 g/h, initial fill 1.5 L of 1.5% dextrose solution). All investigations were preceded by an overnight 2 L 7.5% icodextrin dwell.
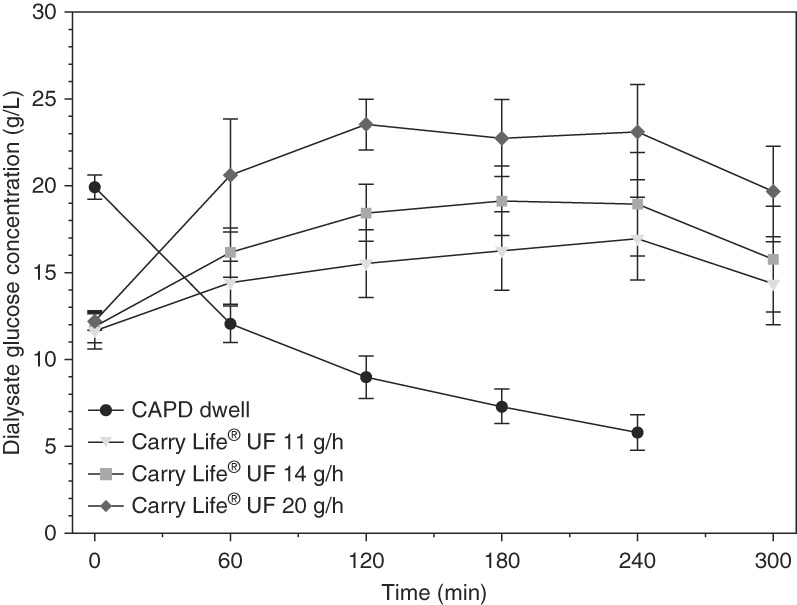
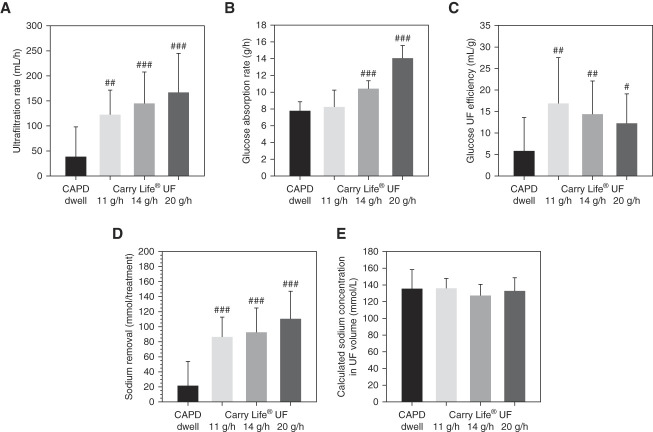
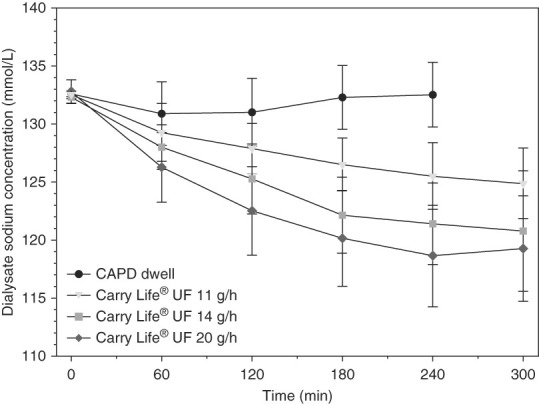
Results: Intraperitoneal glucose concentration increased during the first 1-2 hours of the steady concentration PD treatments and remained stable thereafter. Ultrafiltration rates were significantly higher with steady concentration PD treatments (124±49, 146±63, and 168±78 mL/h with 11, 14, and 20 g/h, respectively, versus 40±60 mL/h with the control dwell). Sodium removal and glucose ultrafiltration efficiency (ultrafiltration volume/gram glucose uptake) were significantly higher with steady concentration PD treatments versus the control dwell, where the 11 g/h glucose dose was most efficient.
Conclusions: Steady concentration PD performed with the Carry Life UF device resulted in higher ultrafiltration rates, more efficient use of glucose (increased ultrafiltration volume/gram glucose absorbed), and greater sodium removal compared with a standard 2.5% dextrose CAPD dwell.
Clinical trial registry name and registration number: A Performance Analysis of the Peritoneal Ultrafiltration (PUF) Achieved With the Carry Life ® UF, NCT03724682 .
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
O. Carlsson and C. De Leon report employment with Triomed AB. J. Hegbrant reports employment with JBA Medical AB; consultancy for Triomed AB; ownership interest in Diaverum AB, LundaTec AB, NorrDia AB, Redsense Medical AB, and Triomed AB; and advisory or leadership roles for Board of Directors of NorrDia AB and Redsense Medical AB. O. Heimbürger reports research funding from AstraZeneca, Baxter, and Triomed; honoraria from AstraZeneca, Baxter Healthcare, Fresenius Medical Care, and Vifor for presentations at company-organized courses; speakers bureau for AstraZeneca; and other interests or relationships as Secretary of Swedish Society of Renal Medicine (2021); and role on Editorial Boards of
Figures

References
-
- Fresenius Medical Care AG & Co. KGaA. Fresenius Medical Care Annual Report 2021 Table 2.20, page 38. 2021. Accessed November 7, 2023. https://www.freseniusmedicalcare.com/fileadmin/data/com/pdf/Media_Center...
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
