

Use of Urea for the Syndrome of Inappropriate Secretion of Antidiuretic Hormone: A Systematic Review
- PMID: 37902751
- PMCID: PMC10616719
- DOI: 10.1001/jamanetworkopen.2023.40313
Use of Urea for the Syndrome of Inappropriate Secretion of Antidiuretic Hormone: A Systematic Review
Abstract
Importance: Hyponatremia and the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) are associated with significant mortality and morbidity. The effectiveness and safety of oral urea for SIADH are still debated.
Objective: To evaluate the efficacy and safety of urea for the treatment of SIADH.
Evidence review: A systematic search of Medline and Embase was conducted for controlled and uncontrolled studies of urea for SIADH in adult patients. The primary outcome was serum sodium concentration after treatment. Secondary outcomes included the proportion of patients with osmotic demyelination syndrome (ODS), intracranial pressure, and resource use such as length of stay.
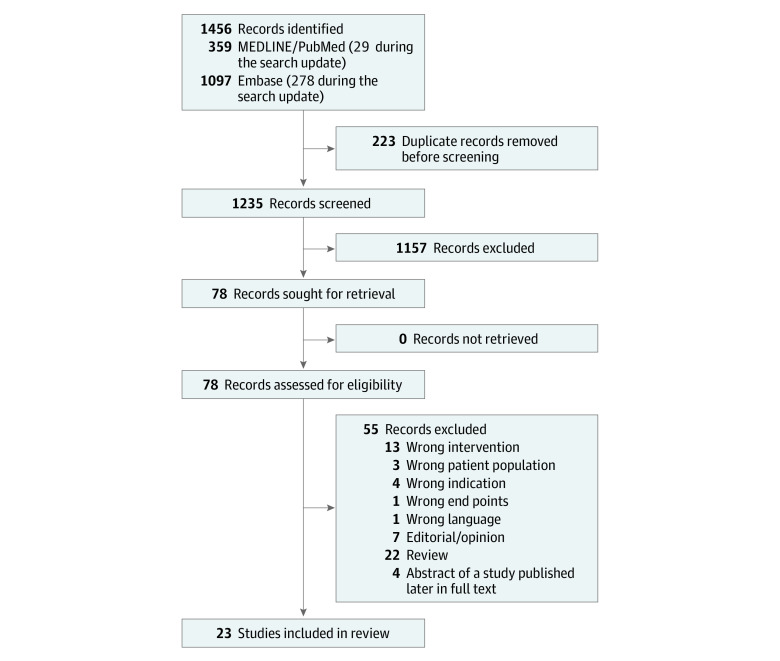
Findings: Twenty-three studies involving 537 patients with SIADH were included, of which 462 were treated with urea. The pooled mean baseline serum sodium was 125.0 mmol/L (95% CI, 122.6-127.5 mmol/L). The median treatment duration with oral urea was 5 days. Urea increased serum sodium concentration by a mean of 9.6 mmol/L (95% CI, 7.5-11.7 mmol/L). The mean increase in serum sodium after 24 hours was 4.9 mmol/L (95% CI, 0.5-9.3 mmol/L). Adverse events were few, mainly consisting of distaste or dysgeusia, and no case of ODS was reported. Resource use was too infrequently reported to be synthesized.
Conclusions and relevance: In this systematic review of the use of urea in SIADH and despite the lack of randomized clinical trials, lower-quality evidence was identified that suggests that urea may be an effective, safe, and inexpensive treatment modality that warrants further exploration.
Conflict of interest statement
References
-
- Kamgar M, Hanna RM, Hasnain H, Khalil D, Wilson JM. Risk of serum sodium overcorrection with V2 antagonists in SIADH and other high risk patients. J Onco-nephrol. 2017;1(3):143-146. doi:10.5301/jo-n.5000025 - DOI
-
- Woudstra J, de Boer MP, Hempenius L, van Roon EN. Urea for hyponatraemia due to the syndrome of inappropriate antidiuretic hormone secretion. Neth J Med. 2020;78(3):125-131. - PubMed
