

Comparison of SP263 and 22C3 immunohistochemistry PD-L1 assays for clinical efficacy of adjuvant atezolizumab in non-small cell lung cancer: results from the randomized phase III IMpower010 trial
- PMID: 37903590
- PMCID: PMC10619123
- DOI: 10.1136/jitc-2023-007047
Comparison of SP263 and 22C3 immunohistochemistry PD-L1 assays for clinical efficacy of adjuvant atezolizumab in non-small cell lung cancer: results from the randomized phase III IMpower010 trial
Abstract
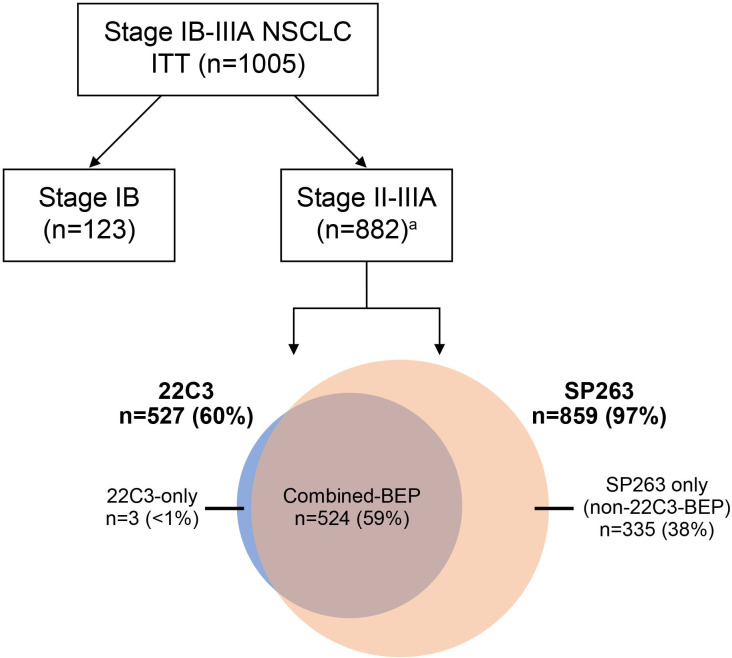
Background: Tumor samples from the phase III IMpower010 study were used to compare two programmed death-ligand 1 (PD-L1) immunohistochemistry assays (VENTANA SP263 and Dako 22C3) for identification of PD-L1 patient subgroups (negative, positive, low, and high expression) and their predictive value for adjuvant atezolizumab compared with best supportive care (BSC) in resectable early-stage non-small cell lung cancer (NSCLC).
Methods: PD-L1 expression was assessed by the SP263 assay, which measured the percentage of tumor cells with any membranous PD-L1 staining, and the 22C3 assay, which scored the percentage of viable tumor cells showing partial or complete membranous PD-L1 staining.
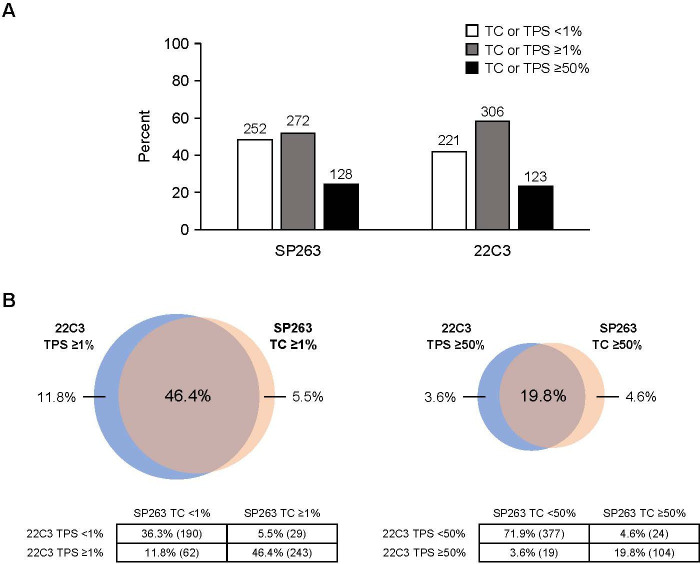
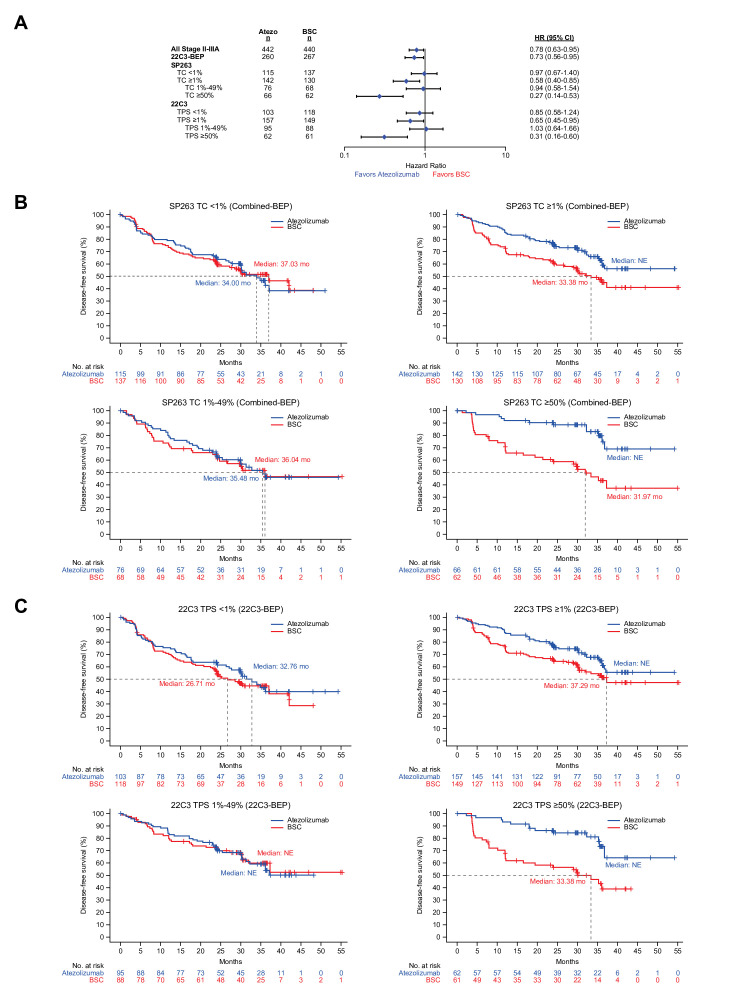
Results: When examining the concordance at the PD-L1-positive threshold (SP263: tumor cell (TC)≥1%; 22C3: tumor proportion score (TPS)≥1%), the results were concordant between assays for 83% of the samples. Similarly, at the PD-L1-high cut-off (SP263: TC≥50%; 22C3: TPS≥50%), the results were concordant between assays for 92% of samples. The disease-free survival benefit of atezolizumab over BSC was comparable between assays for PD-L1-positive (TC≥1% by SP263: HR, 0.58 (95% CI: 0.40 to 0.85) vs TPS≥1% by 22C3: HR, 0.65 (95% CI: 0.45 to 0.95)) and PD-L1-high (TC≥50% by SP263: HR, 0.27 (95% CI: 0.14 to 0.53) vs TPS≥50% by 22C3: HR, 0.31 (95% CI: 0.16 to 0.60)) subgroups.
Conclusions: The SP263 and 22C3 assays showed high concordance and a comparable clinical predictive value of atezolizumab at validated PD-L1 thresholds, suggesting that both assays can identify patients with early-stage NSCLC most likely to experience benefit from adjuvant atezolizumab.
Trial registration number: NCT02486718.
Keywords: immune checkpoint inhibitors; immunohistochemistry; non-small cell lung cancer; programmed cell death 1 receptor; tumor biomarkers.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: CZ reports consulting fees from Innovent Biologics, Qilu, Hengrui, and TopAlliance Biosciences Inc; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Eli Lilly China, Sanofi, Boehringer Ingelheim, Roche, MSD, Qilu, Hengrui, Innovent Biologics, C-Stone LUYE Pharma, TopAlliance Biosciences Inc, Amoy Diagnostics, and AnHeart. MS reports employment by Genentech and stockholding in Roche. HX reports stockholding in Roche as a former Roche employee. EF reports grants or contracts from Merck Healthcare KGaA and Fundación Merck Salud; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Amgen, AstraZeneca, Bristol Myers Squibb, Eli Lilly, F. Hoffman-La Roche, Janssen, Medical Trends, Medscape, Merck Serono, Merck Sharp & Dohme, PeerVoice, Pfizer, Sanofi, Takeda, and Touch Oncology; and is an independent member of the board for Grífols. HW reports grants or contracts from ACEA Biosciences, Arrys Therapeutics, AstraZeneca/Medimmune, Bristol Myers Squibb, Clovis Oncology, Genentech/Roche, Merck, Novartis, SeaGen, Xcovery, and Helsinn; participation on a data safety monitoring board or advisory board for AstraZeneca, Janssen, Daiichi Sankyo, Blueprint, Mirati, Merck, and Genentech/Roche; and leadership or fiduciary role in other board, society, committee, or advocacy group (paid or unpaid) for International Association for the Study of Lung Cancer (IASLC) and ECOG-ARIN. MR reports consulting fees from Amgen, AstraZeneca, BeiGene, Bristol Myers Squibb, Boehringer-Ingelheim, Daiichi Sankyo, GSK, Mirati, Merck, MSD, Novartis, Pfizer, Sanofi, and Roche; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Amgen, AstraZeneca, BeiGene, Bristol Myers Squibb, Boehringer Ingelheim, Daiichi Sankyo, GSK, Mirati, Merck, MSD, Novartis, Pfizer, Sanofi, and Roche; support for attending meetings and/or travel from Amgen, AstraZeneca, BeiGene, Bristol Myers Squibb, Boehringer Ingelheim, Daiichi Sankyo, GSK, Mirati, Merck, MSD, Novartis, Pfizer, Sanofi, and Roche; and participation on a data safety monitoring board or advisory board for Sanofi and Daiichi Sankyo. SO reports grants or contracts from AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Chugai Pharmaceuticals, Daiichi Sankyo, Ono Pharmaceutical, Pfizer, MSD, Sanofi, Taiho, and Takeda. Hiroshi Tanaka reports grants or contracts from Chugai Pharmaceuticals, AstraZeneca, MSD, Ono Pharmaceutical, and Bristol Myers Squibb; and honoraria for Chugai Pharmaceuticals, AstraZeneca, MSD, Ono Pharmaceutical, and Bristol Myers Squibb. SLM reports support from Genentech as a research site for this trial. EB reports employment by Genentech and stockholding in Roche. BG reports employment by Genentech and stockholding in Roche. VM reports employment by Roche and stockholding in Roche. MB reports employment by Genentech and stockholding in Roche. MM reports being a former employee of Roche/Genentech. WZ reports employment by Roche and stockholding in Roche. MDT reports stock or stock options as a former employee of Roche/Genentech. SN reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca, Amgen, Boehringer Ingelheim, Roche, Pfizer, Takeda, Novartis, Sanofi, Janssen, and GSK; and participation on a data safety monitoring board or advisory board for AstraZeneca, Amgen, Boehringer Ingelheim, Roche, Pfizer, Takeda, Novartis, Sanofi, Janssen, and GSK. NA, RL, AK and JH declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials