

Epidemiology and disease burden of patients requiring neurocritical care: a Brazilian multicentre cohort study
- PMID: 37903826
- PMCID: PMC10616165
- DOI: 10.1038/s41598-023-44261-w
Epidemiology and disease burden of patients requiring neurocritical care: a Brazilian multicentre cohort study
Abstract
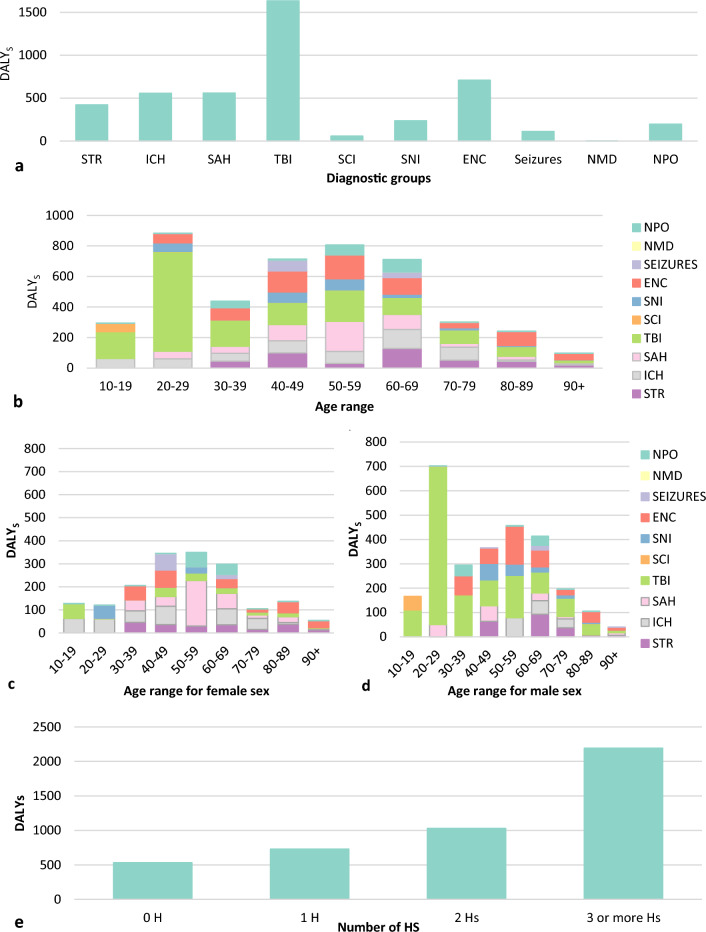
Acute neurological emergencies are highly prevalent in intensive care units (ICUs) and impose a substantial burden on patients. This study aims to describe the epidemiology of patients requiring neurocritical care in Brazil, and their differences based on primary acute neurological diagnoses and to identify predictors of mortality and unfavourable outcomes, along with the disease burden of each condition at intensive care unit admission. This prospective cohort study included patients requiring neurocritical care admitted to 36 ICUs in four Brazilian regions who were followed for 30 days or until ICU discharge (Aug-Sep in 2018, 1 month). Of 4245 patients admitted to the participating ICUs, 1194 (28.1%) were patients with acute neurological disorders requiring neurocritical care and were included. Patients requiring neurocritical care had a mean mortality rate 1.7 times higher than ICU patients not requiring neurocritical care (17.21% versus 10.1%, respectively). Older age, emergency admission, higher number of potential secondary injuries, and worse APACHE II, SAPS III, SOFA, and Glasgow coma scale scores on ICU admission are independent predictors of mortality and poor outcome among patients with acute neurological diagnoses. The estimated total DALYs were 4482.94 in the overall cohort, and the diagnosis with the highest DALYs was traumatic brain injury (1634.42). Clinical, epidemiological, treatment, and ICU outcome characteristics vary according to the primary neurologic diagnosis. Advanced age, a lower GCS score and a higher number of potential secondary injuries are independent predictors of mortality and unfavourable outcomes in patients requiring neurocritical care. The findings of this study are essential to guide education policies, prevention, and treatment of severe acute neurocritical diseases.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Epimed, M. & AMIB. Adult ICU Profile by diagnoses. Epimed Monitor—data from 01/01/2010 to 06/30/2023. UTIs Brasileiras - the National Intensive Care Register in Brazil.https://www.utisbrasileiras.com/diagnosticos/ (2023).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
