

Prevalence of multiple long-term conditions (multimorbidity) in England: a whole population study of over 60 million people
- PMID: 37905525
- PMCID: PMC11046366
- DOI: 10.1177/01410768231206033
Prevalence of multiple long-term conditions (multimorbidity) in England: a whole population study of over 60 million people
Abstract
Objectives: To determine the prevalence of multiple long-term conditions (MLTC) at whole English population level, stratifying by age, sex, socioeconomic status and ethnicity.
Design: A whole population study.
Setting: Individuals registered with a general practice in England and alive on 31 March 2020.
Participants: 60,004,883 individuals.
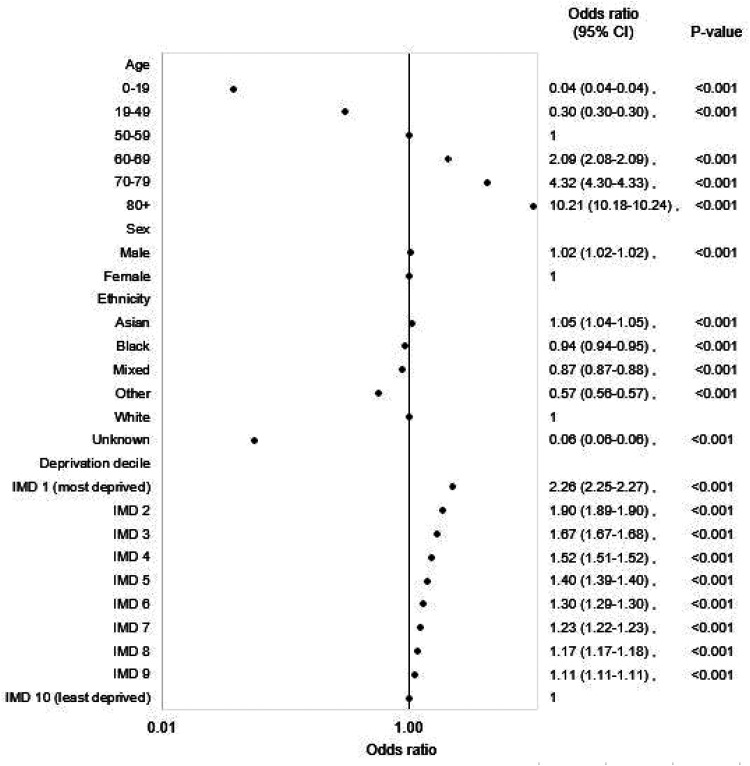
Main outcome measures: MLTC prevalence, defined as two or more of 35 conditions derived from a number of national patient-level datasets. Multivariable logistic regression was used to assess the independent associations of age, sex, ethnicity and deprivation decile with odds of MLTC.
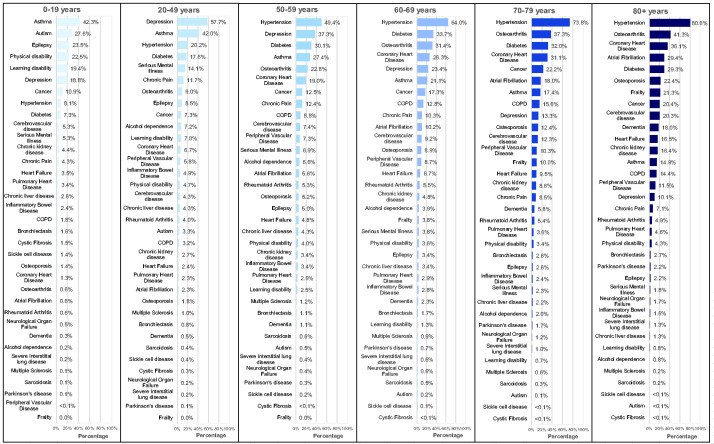
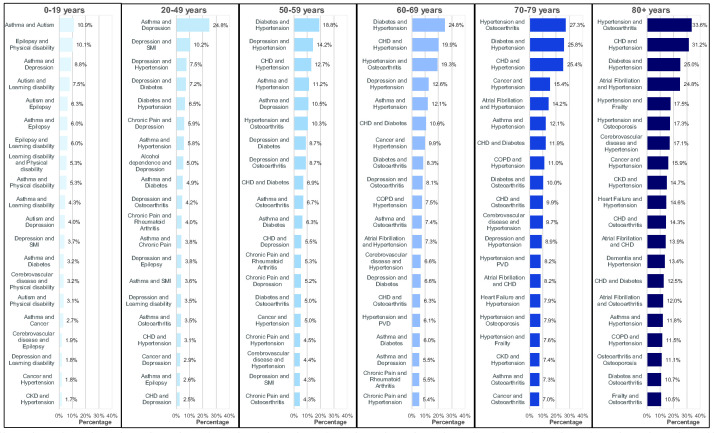
Results: The overall prevalence of MLTC was 14.8% (8,878,231), varying from 0.9% (125,159) in those aged 0-19 years to 68.2% (1,905,979) in those aged 80 years and over. In multivariable regression analyses, compared with the 50-59 reference group, the odds ratio was 0.04 (95% confidence interval (CI): 0.04-0.04; p < 0.001) for those aged 0-19 years and 10.21 (10.18-10.24; p < 0.001) for those aged 80 years and over. Odds were higher for men compared with women, 1.02 (1.02-1.02; p < 0.001), for the most deprived decile compared with the least deprived, 2.26 (2.25-2.27; p < 0.001), and for Asian ethnicity compared with those of white ethnicity, 1.05 (1.04-1.05; p < 0.001). Odds were lower for black, mixed and other ethnicities (0.94 (0.94-0.95) p < 0.001, 0.87 (0.87-0.88) p < 0.001 and 0.57 (0.56-0.57) p < 0.001, respectively). MLTC for persons aged 0-19 years were dominated by asthma, autism and epilepsy, for persons aged 20-49 years by depression and asthma, for persons aged 50-59 years by hypertension and depression and for those aged 60 years and older, by cardiometabolic factors and osteoarthritis. There were large numbers of combinations of conditions in each age group ranging from 5936 in those aged 0-19 years to 205,534 in those aged 80 years and over.
Conclusions: While this study provides useful insight into the burden across the English population to assist health service delivery planning, the heterogeneity of MLTC presents challenges for delivery optimisation.
Keywords: Epidemiologic studies; epidemiology; health policy; health service research; medical management; quality improvement.
Conflict of interest statement
JV is National Clinical Director for Diabetes and Obesity at NHS England. KK is National National Institute for Health Research (NIHR) Applied Research Collaboration Lead for MLTC and Director of NIHR Global Research Centre for MLTC. NH, EBT and RDR are employed by Outcomes Based Healthcare, which receives funding from NHS organisations (including NHS England) for providing analytical services. JM is NIHR Clinical Research Network (CRN) Project Lead for MLTC and Head of Cluster A, NIHR CRN Coordinating Centre. KR is NIHR Clinical Research Network Project Manager for MLTC.
Figures
References
-
- Head A, Fleming K, Kypridemos C, Schofield P, Pearson-Stuttard J, O’Flaherty M. Inequalities in incident and prevalent multimorbidity in England, 2004–19: a population-based, descriptive study. Lancet Healthy Longev 2021; 2: e489–497. - PubMed
-
- National Institute for Health and Care Excellence. Multimorbidity: clinical assessment and management NICE guideline. 2016. See www.nice.org.uk/guidance/ng56/resources/multimorbidity-clinical-assessme... (last checked 19 August 2022).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
