

Post-acute ischemic stroke hyperglycemia aggravates destruction of the blood-brain barrier
- PMID: 37905884
- PMCID: PMC11467929
- DOI: 10.4103/1673-5374.385851
Post-acute ischemic stroke hyperglycemia aggravates destruction of the blood-brain barrier
Abstract
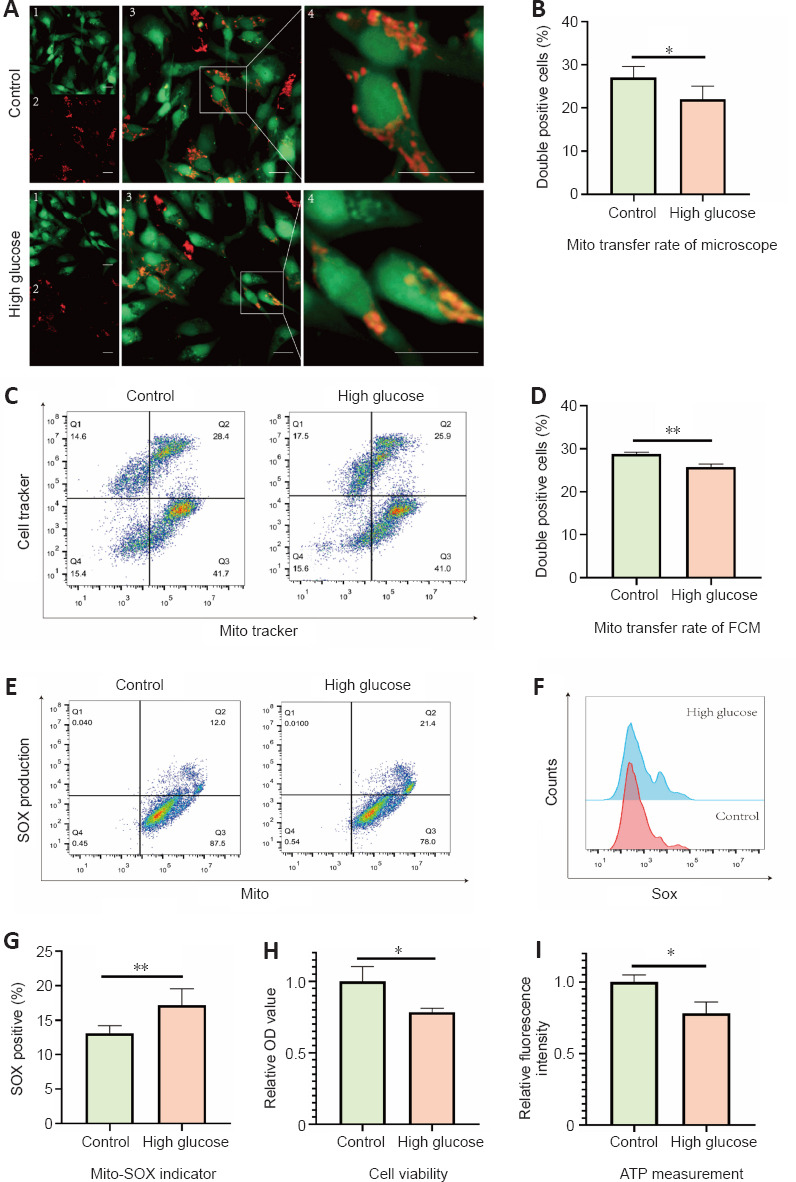
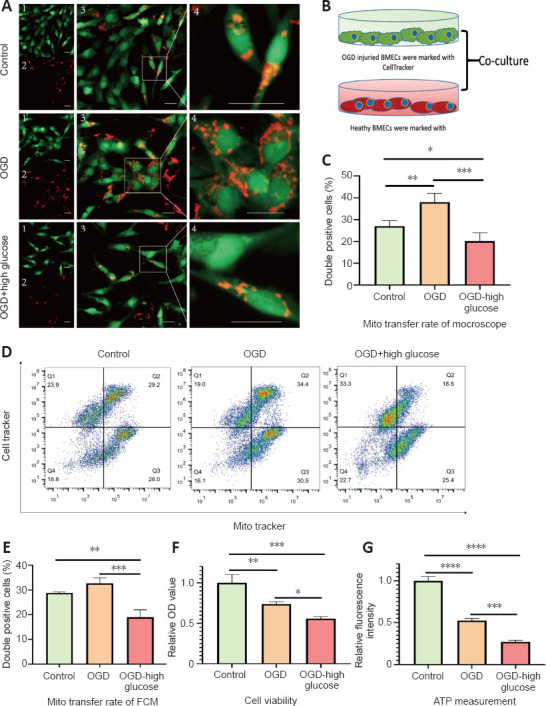
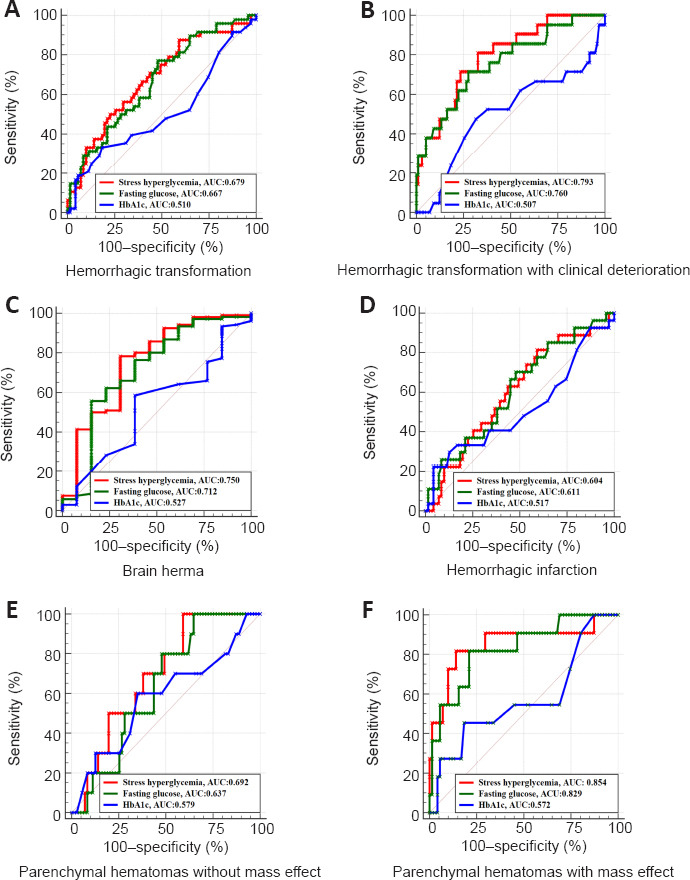
Post-acute ischemic stroke hyperglycemia increases the risk of hemorrhagic transformation, which is associated with blood-brain barrier disruption. Brain microvascular endothelial cells are a major component of the blood-brain barrier. Intercellular mitochondrial transfer has emerged as a novel paradigm for repairing cells with mitochondrial dysfunction. In this study, we first investigated whether mitochondrial transfer exists between brain microvascular endothelial cells, and then investigated the effects of post-acute ischemic stroke hyperglycemia on mitochondrial transfer between brain microvascular endothelial cells. We found that healthy brain microvascular endothelial cells can transfer intact mitochondria to oxygen glucose deprivation-injured brain microvascular endothelial cells. However, post-oxygen glucose deprivation hyperglycemia hindered mitochondrial transfer and exacerbated mitochondrial dysfunction. We established an in vitro brain microvascular endothelial cell model of the blood-brain barrier. We found that post-acute ischemic stroke hyperglycemia reduced the overall energy metabolism levels of brain microvascular endothelial cells and increased permeability of the blood-brain barrier. In a clinical study, we retrospectively analyzed the relationship between post-acute ischemic stroke hyperglycemia and the severity of hemorrhagic transformation. We found that post-acute ischemic stroke hyperglycemia serves as an independent predictor of severe hemorrhagic transformation. These findings suggest that post-acute ischemic stroke hyperglycemia can aggravate disruption of the blood-brain barrier by inhibiting mitochondrial transfer.
Conflict of interest statement
Figures





References
-
- Baird TA, Parsons MW, Phan T, Butcher KS, Desmond PM, Tress BM, Colman PG, Chambers BR, Davis SM. Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome. Stroke. (2003);34:2208–2214. - PubMed
-
- Berger C, Fiorelli M, Steiner T, Schäbitz WR, Bozzao L, Bluhmki E, Hacke W, von Kummer R. Hemorrhagic transformation of ischemic brain tissue:asymptomatic or symptomatic? Stroke. (2001);32:1330–1335. - PubMed
LinkOut - more resources
Full Text Sources
