

Incidence, Microbiological Studies, and Factors Associated With Prosthetic Joint Infection After Total Knee Arthroplasty
- PMID: 37906194
- PMCID: PMC10618849
- DOI: 10.1001/jamanetworkopen.2023.40457
Incidence, Microbiological Studies, and Factors Associated With Prosthetic Joint Infection After Total Knee Arthroplasty
Abstract
Importance: Despite the frequency of total knee arthroplasty (TKA) and clinical implications of prosthetic joint infections (PJIs), knowledge gaps remain concerning the incidence, microbiological study results, and factors associated with these infections.
Objectives: To identify the incidence rates, organisms isolated from microbiological studies, and patient and surgical factors of PJI occurring early, delayed, and late after primary TKA.
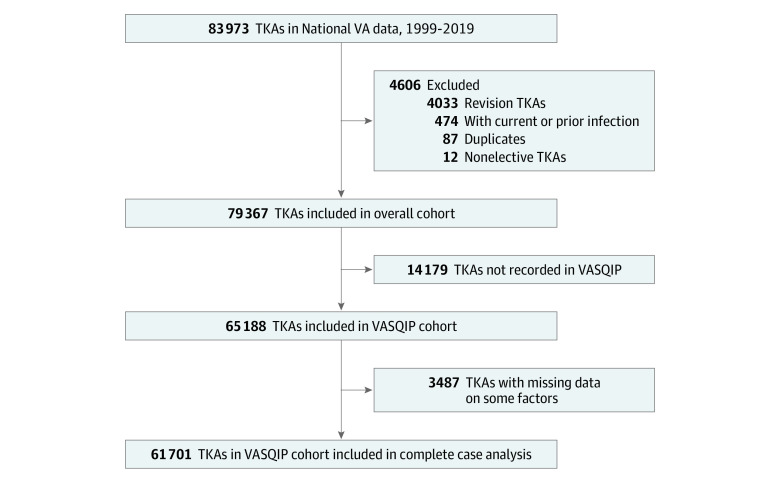
Design, setting, and participants: This cohort study obtained data from the US Department of Veterans Affairs (VA) Corporate Data Warehouse on patients who underwent elective primary TKA in the VA system between October 1, 1999, and September 30, 2019, and had at least 1 year of care in the VA prior to TKA. Patients who met these criteria were included in the overall cohort, and patients with linked Veterans Affairs Surgical Quality Improvement Program (VASQIP) data composed the VASQIP cohort. Data were analyzed between December 9, 2021, and September 18, 2023.
Exposures: Primary TKA as well as demographic, clinical, and perioperative factors.
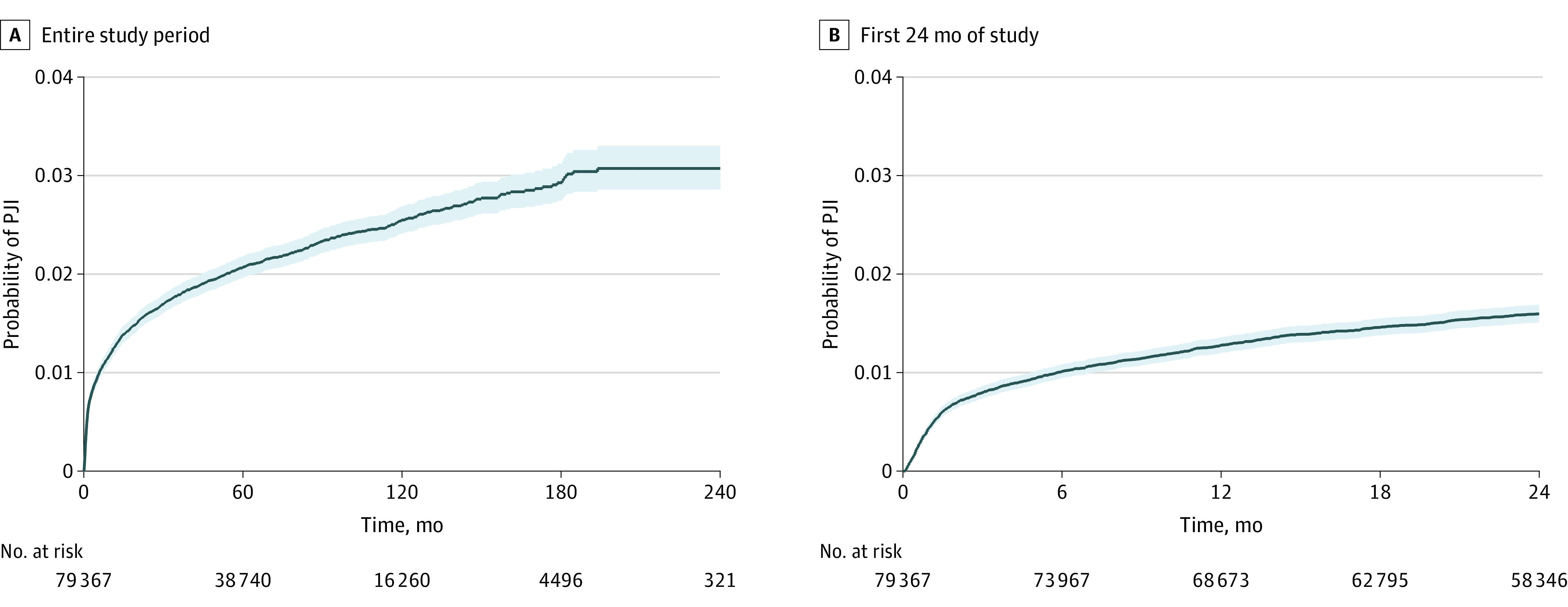
Main outcomes and measures: Incident hospitalization with early, delayed, or late PJI. Incidence rate (events per 10 000 person-months) was measured in 3 postoperative periods: early (≤3 months), delayed (between >3 and ≤12 months), and late (>12 months). Unadjusted Poisson regression was used to estimate incidence rate ratios (IRRs) with 95% CIs of early and delayed PJI compared with late PJI. The frequency of organisms isolated from synovial or operative tissue culture results of PJIs during each postoperative period was identified. A piecewise exponential parametric survival model was used to estimate IRRs with 95% CIs associated with demographic and clinical factors in each postoperative period.
Results: The 79 367 patients (median (IQR) age of 65 (60-71) years) in the overall cohort who underwent primary TKA included 75 274 males (94.8%). A total of 1599 PJIs (2.0%) were identified. The incidence rate of PJI was higher in the early (26.8 [95% CI, 24.8-29.0] events per 10 000 person-months; IRR, 20.7 [95% CI, 18.5-23.1]) and delayed periods (5.4 [95% CI, 4.9-6.0] events per 10 000 person-months; IRR, 4.2 [95% CI, 3.7-4.8]) vs the late postoperative period (1.3 events per 10 000 person-months). Staphylococcus aureus was the most common organism isolated overall (489 [33.2%]); however, gram-negative infections were isolated in 15.4% (86) of early PJIs. In multivariable analyses, hepatitis C virus infection, peripheral artery disease, and autoimmune inflammatory arthritis were associated with PJI across all postoperative periods. Diabetes, chronic kidney disease, and obesity (body mass index of ≥30) were not associated factors. Other period-specific factors were identified.
Conclusions and relevance: This cohort study found that incidence rates of PJIs were higher in the early and delayed vs late post-TKA period; there were differences in microbiological cultures and factors associated with each postoperative period. These findings have implications for postoperative antibiotic use, stratification of PJI risk according to postoperative time, and PJI risk factor modification.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
