

Ocrelizumab exposure in relapsing-remitting multiple sclerosis: 10-year analysis of the phase 2 randomized clinical trial and its extension
- PMID: 37906326
- PMCID: PMC10827899
- DOI: 10.1007/s00415-023-11943-4
Ocrelizumab exposure in relapsing-remitting multiple sclerosis: 10-year analysis of the phase 2 randomized clinical trial and its extension
Abstract
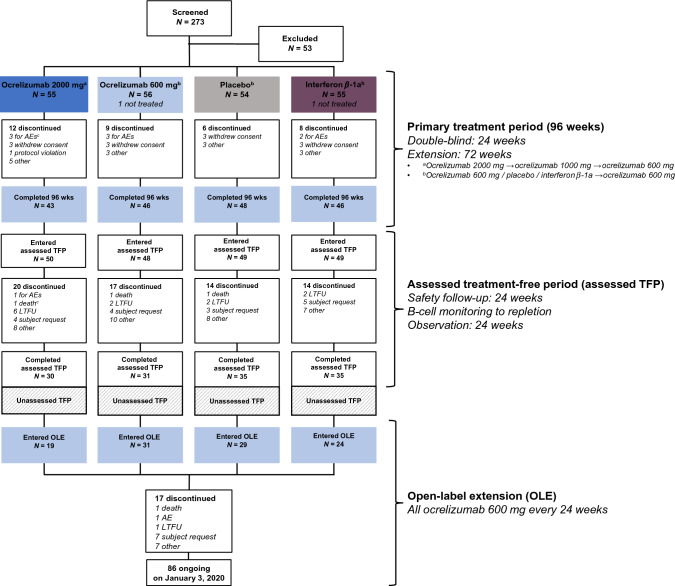
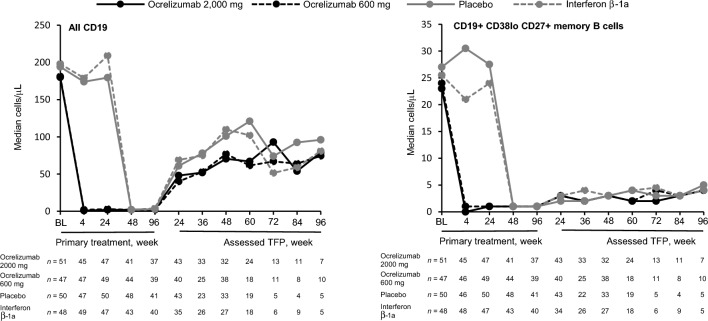
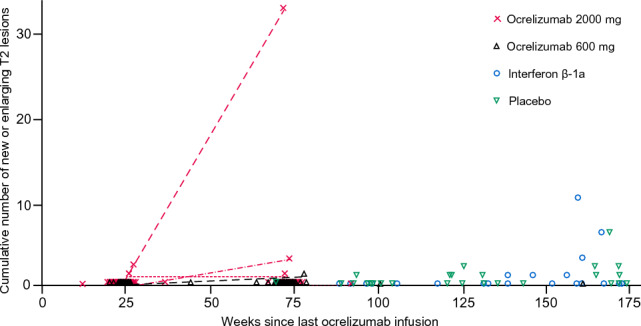
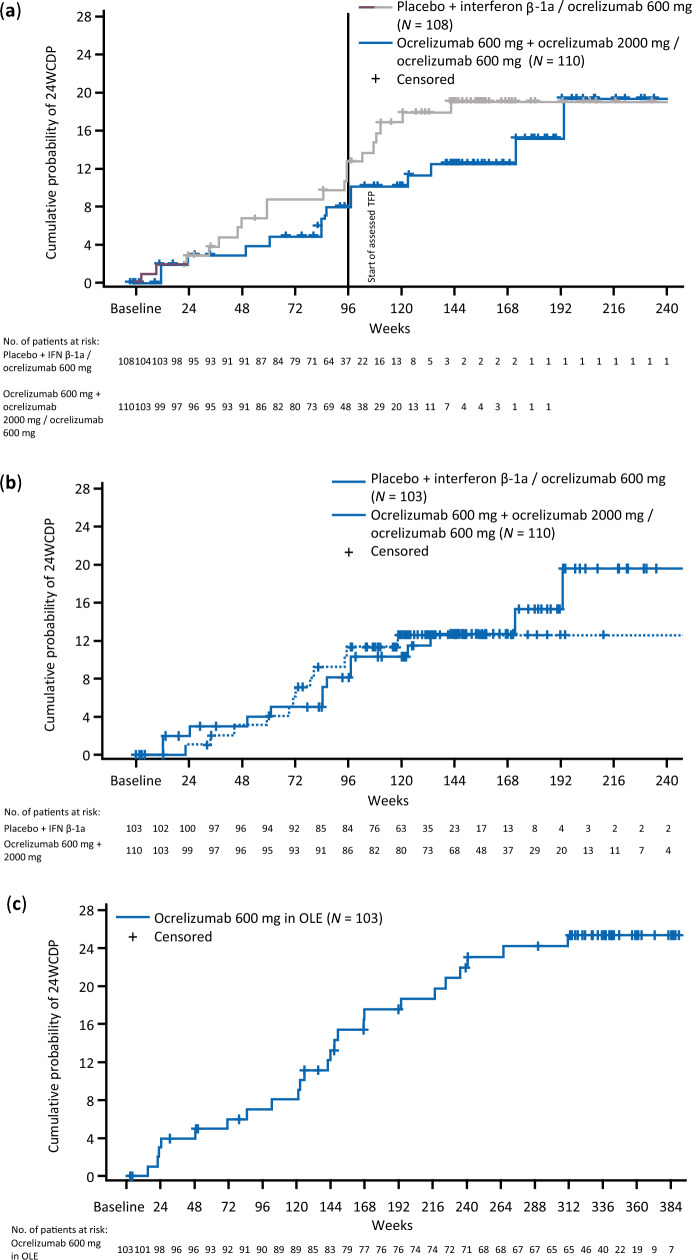
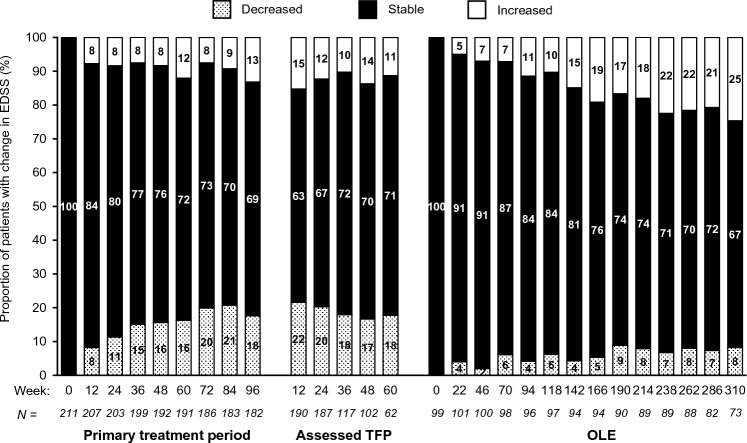
Open-label extension (OLE) studies help inform long-term safety and efficacy of disease-modifying therapies in multiple sclerosis (MS). We report exploratory analyses from a phase 2 trial on the longest follow-up to date of ocrelizumab-treated patients with relapsing-remitting MS (RRMS). The primary treatment period (PTP) comprised four 24-week treatment cycles; participants were randomized to double-blind ocrelizumab (2000 mg or 600 mg), placebo, or interferon β-1a (open label) for one cycle, then dose-blinded ocrelizumab 1000 mg or 600 mg for the remaining cycles. The PTP was followed by consecutive assessed and unassessed treatment-free periods (TFPs) and then the OLE (ocrelizumab 600 mg every 24 weeks). Safety and efficacy were prospectively assessed. Of 220 participants randomized, 183 (84%) completed the PTP. After the TFP, 103 entered OLE (median OLE ocrelizumab exposure 6.5 years). Most common adverse events across all periods were infusion-related reactions. MRI activity, annualized relapse rate, and confirmed disability progression (CDP) rates remained low throughout. During the assessed TFP, there was a trend toward less and later B-cell repletion, and later CDP, for patients randomized to ocrelizumab; MRI activity was observed in 16.3% of patients, the earliest 24 weeks after the last ocrelizumab dose. This is the longest follow-up of ocrelizumab-treated patients with RRMS, with no new safety signals emerging during an observation period from 2008 to 2020. Results reinforce the sustained efficacy of long-term ocrelizumab. Reduced disease activity was maintained following interruption of 6-month dosing cycles, with no evidence of rebound.
Keywords: Disease-modifying therapies; Multiple sclerosis; Ocrelizumab; Safety.
© 2023. The Author(s).
Figures
References
-
- Wolinsky JS, Arnold DL, Brochet B, et al. Long-term follow-up from the ORATORIO trial of ocrelizumab for primary progressive multiple sclerosis: a post-hoc analysis from the ongoing open-label extension of the randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2020;19(12):998–1009. doi: 10.1016/S1474-4422(20)30342-2. - DOI - PubMed
