

Primary progressive aphasia: six questions in search of an answer
- PMID: 37906327
- PMCID: PMC10827918
- DOI: 10.1007/s00415-023-12030-4
Primary progressive aphasia: six questions in search of an answer
Abstract
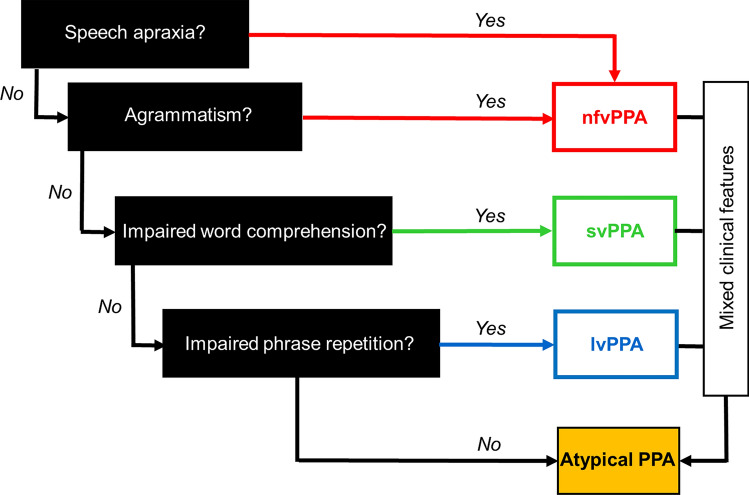
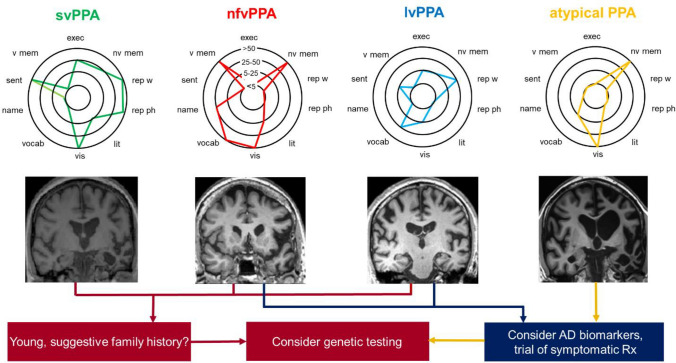
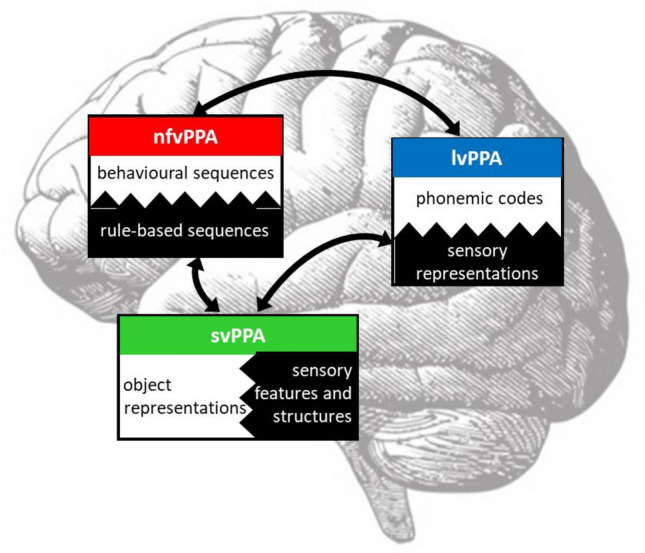
Here, we review recent progress in the diagnosis and management of primary progressive aphasia-the language-led dementias. We pose six key unanswered questions that challenge current assumptions and highlight the unresolved difficulties that surround these diseases. How many syndromes of primary progressive aphasia are there-and is syndromic diagnosis even useful? Are these truly 'language-led' dementias? How can we diagnose (and track) primary progressive aphasia better? Can brain pathology be predicted in these diseases? What is their core pathophysiology? In addition, how can primary progressive aphasia best be treated? We propose that pathophysiological mechanisms linking proteinopathies to phenotypes may help resolve the clinical complexity of primary progressive aphasia, and may suggest novel diagnostic tools and markers and guide the deployment of effective therapies.
Keywords: Alzheimer’s disease; Frontotemporal dementia; Logopenic aphasia; Primary progressive aphasia; Semantic dementia.
© 2023. The Author(s).
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
