

Post-Stroke Spastic Movement Disorder and Botulinum Toxin A Therapy: Early Detection And Early Injection
- PMID: 37907224
- PMCID: PMC10620487
- DOI: 10.5535/arm.23108
Post-Stroke Spastic Movement Disorder and Botulinum Toxin A Therapy: Early Detection And Early Injection
Abstract
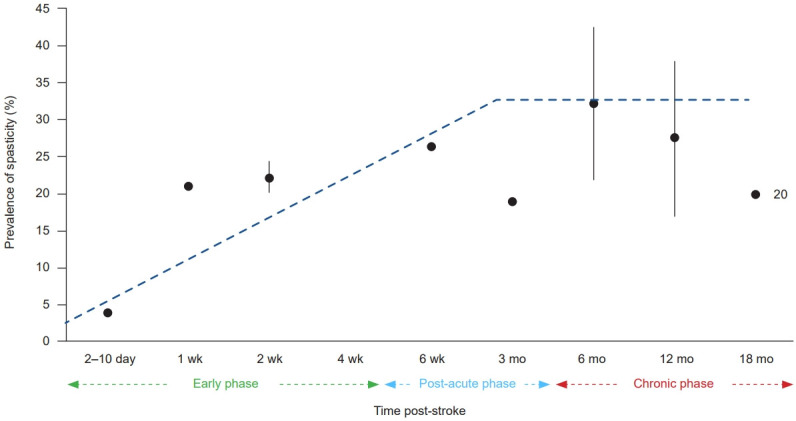
Post-stroke spastic movement disorder (PS-SMD) develops in up to 40% of stroke survivors after a first ever stroke within the first year. Chronic PS-SMD is often associated with severe disabilities and complications, emphasizing the importance of its early recognition and early adequate management. Extensive research has aimed to accurately predict and sensitively detect a PS-SMD. Symptomatic therapies include conventional rehabilitation and local intramuscular injections of botulinum toxin A (BoNT-A). The latter is widely used, but primarily in the chronic phase of stroke. However, recent studies have shown the safety and efficacy of BoNT-A therapy even in the acute phase and early sub-acute phase after stroke, i.e., within three months post-stroke, leading to an improved long-term outcome in stroke rehabilitation. Local BoNT-A injections evolve as the primary approach in focal, multifocal, and segmental chronic or acute/subacute PS-SMD. Patients at high risk for or manifest PS-SMD should be identified by an early spasticity risk assessment. By doing so, PS-SMD can be integral part of the patient-centered goal-setting process of a multiprofessional spasticity-experienced team. The benefit of an early PS-SMD treatment by BoNT-A should predominate putative degenerative muscle changes due to long-term BoNT-A therapy by far. This, as early treatment effectively avoids complications typically associated with a PS-SMD, i.e., contractures, pain, skin lesions. The management of PS-SMD requires a comprehensive and multidisciplinary approach. Early assessment, patient-centered goal setting, early intervention, and early use of BoNT-A therapy prevents from PS-SMD complications and may improve rehabilitation outcome after stroke.
Keywords: Botulinum toxin; Movement disorder; Rehabilitation; Spastic; Stroke.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Wissel J, Manack A, Brainin M. Toward an epidemiology of poststroke spasticity. Neurology. 2013;80(3 Suppl 2):S13–9. - PubMed
-
- Wissel J, Ri S. Assessment, goal setting, and botulinum neurotoxin a therapy in the management of post-stroke spastic movement disorder: updated perspectives on best practice. Expert Rev Neurother. 2022;22:27–42. - PubMed
-
- Platz T, Wissel J, Donauer E, Vogel M, Tholen R, Lehmler L. [S2k: treatment of spastic syndromes] [Internet] Deutsche Gesellschaft für Neurologie. 2018 [cited 2023 Jul 13]. Available from: https://register.awmf.org/assets/guidelines/030-078k_S2k_Therapie_spasti.... German.
-
- Mills PB, Phadke CP, Boulias C, Dukelow SP, Ismail F, McNeil SM, et al. Spasticity management teams, evaluations, and tools: a Canadian cross-sectional survey. Can J Neurol Sci. 2022. doi: 10.1017/cjn.2022.326. [Epub ahead of print] - PubMed
LinkOut - more resources
Full Text Sources
