

Comparison of anterior column reconstruction techniques after en bloc spondylectomy: a finite element study
- PMID: 37907570
- PMCID: PMC10618450
- DOI: 10.1038/s41598-023-45736-6
Comparison of anterior column reconstruction techniques after en bloc spondylectomy: a finite element study
Abstract
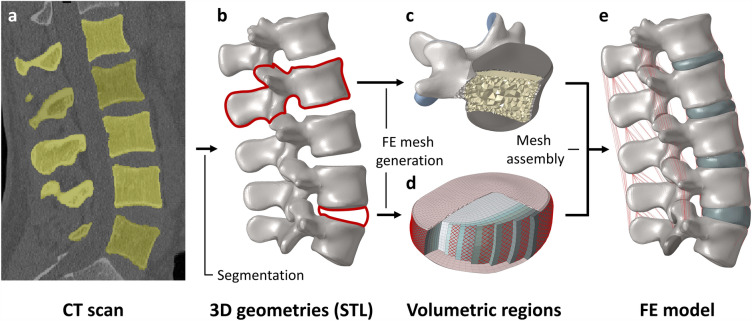
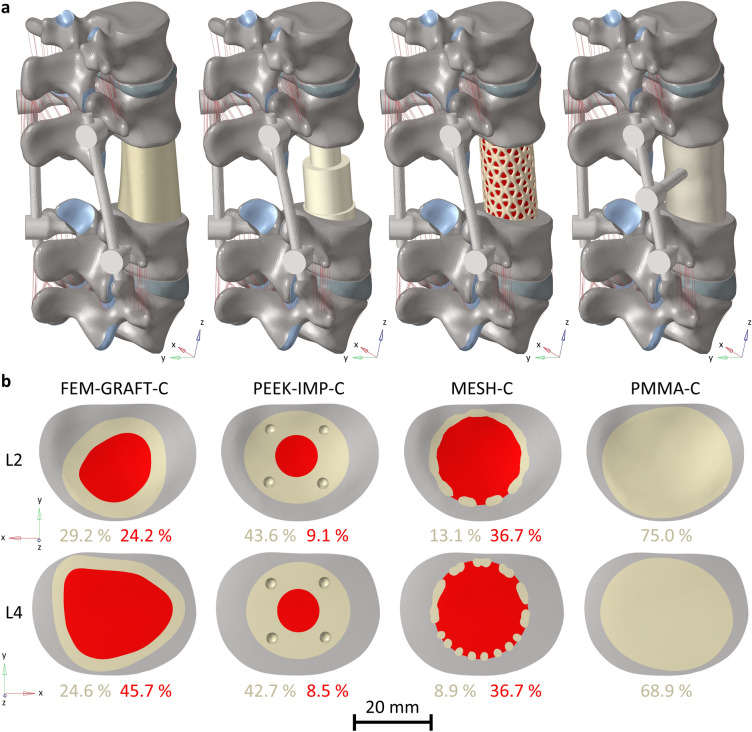
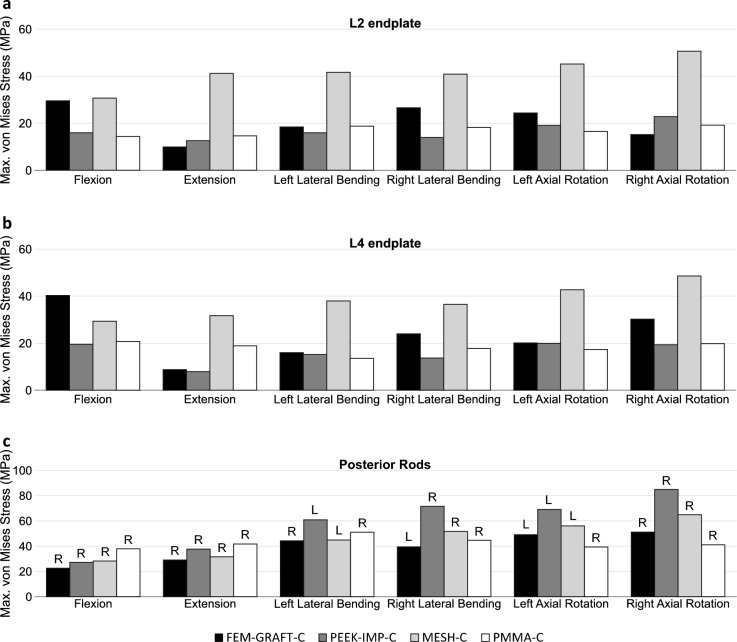
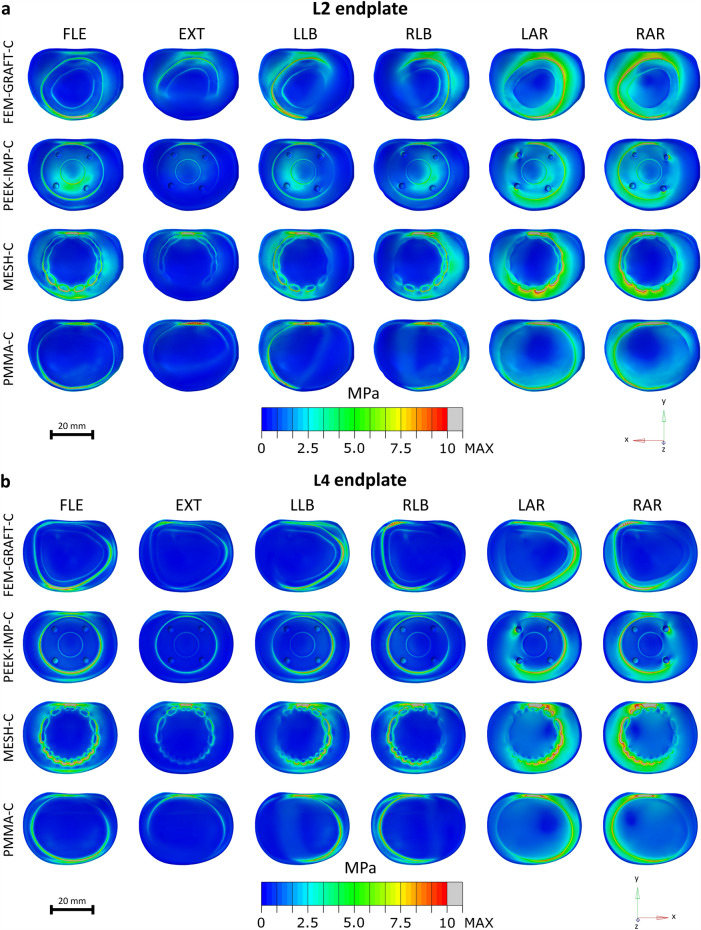
Total en bloc spondylectomy (TES) effectively treats spinal tumors. The surgery requires a vertebral body replacement (VBR), for which several solutions were developed, whereas the biomechanical differences between these devices still need to be completely understood. This study aimed to compare a femur graft, a polyetheretherketone implant (PEEK-IMP-C), a titan mesh cage (MESH-C), and a polymethylmethacrylate replacement (PMMA-C) using a finite element model of the lumbar spine after a TES of L3. Several biomechanical parameters (rotational stiffness, segmental range of motion (ROM), and von Mises stress) were assessed to compare the VBRs. All models provided adequate initial stability by increasing the rotational stiffness and decreasing the ROM between L2 and L4. The PMMA-C had the highest stiffness for flexion-extension, lateral bending, and axial rotation (215%, 216%, and 170% of intact model), and it had the lowest segmental ROM in the instrumented segment (0.2°, 0.5°, and 0.7°, respectively). Maximum endplate stress was similar for PMMA-C and PEEK-IMP-C but lower for both compared to MESH-C across all loading directions. These results suggest that PMMA-C had similar or better primary spinal stability than other VBRs, which may be related to the larger contact surface and the potential to adapt to the patient's anatomy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Szava, J.; Maros, T.; Gsugudean, K. Beitrage zur radicalen chirurgischen Behandlung der Wirbelneoplasmen und die Wiederherstellung der Wirbelsaule nach einer Vertebrectomie. Zentr. Blatt Chir 247–256 (1959). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
