

Combination of genomic instability score and TP53 status for prognosis prediction in lung adenocarcinoma
- PMID: 37907595
- PMCID: PMC10618567
- DOI: 10.1038/s41698-023-00465-x
Combination of genomic instability score and TP53 status for prognosis prediction in lung adenocarcinoma
Abstract
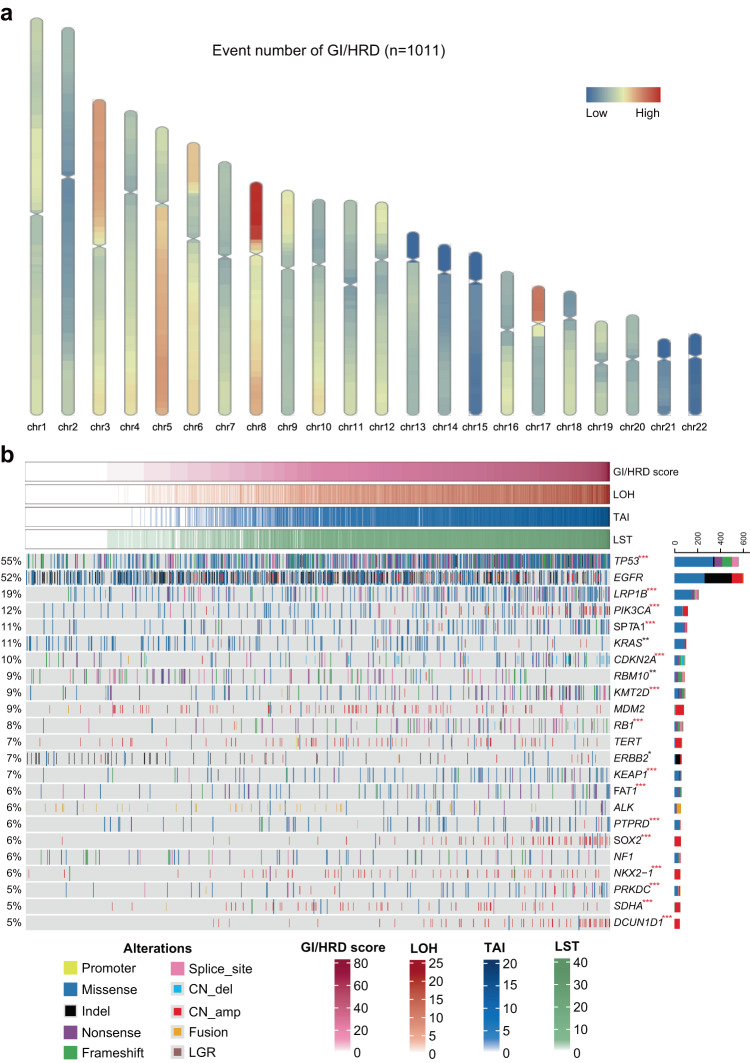
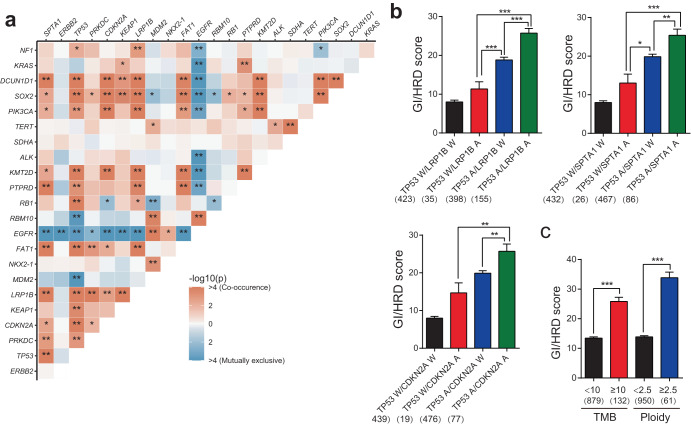
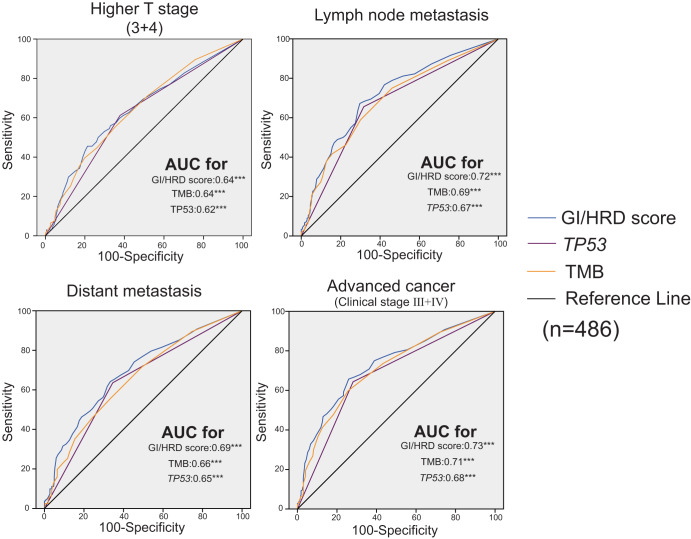
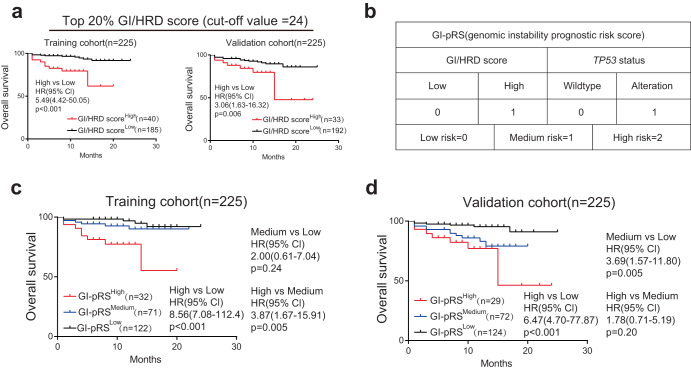
The genomic instability (GI) /homologous recombination deficiency (HRD) score, calculated as the sum of the events of loss of heterozygosity (LOH), large-scale state transition (LST) and telomere allele imbalance (TAI), is used to guide the choice of treatment in several cancers, but its relationship with genomic features, clinicopathological characteristics and prognosis in lung cancer is poorly understood, which could lead to population bias in prospective studies. We retrospectively analyzed 1011 lung cancer patients whose tumor samples were successfully profiled by high-throughput sequencing panel including GI/HRD score. Alterations of many cancer suppressor genes were associated with higher GI/HRD scores, biallelic inactivation of TP53 was correlated with a high GI/HRD score. A combination of two gene alterations exhibited a higher GI/HRD scores than single gene alterations. The GI/HRD score was associated with advanced stages in lung adenocarcinoma but not in lung squamous cell carcinoma. Furthermore, patients with higher GI/HRD scores had significantly shorter overall survival and progression-free survival than patients with lower GI/HRD scores. Finally, patients with a combination of a higher GI/HRD scores and TP53 alteration exhibited an extremely poor prognosis compared with patients with a lower GI/HRD scores and wild-type TP53 (overall survival, training cohort, hazard ratio (HR) = 8.56, P < 0.001; validation cohort, HR = 6.47, P < 0.001; progression-free survival, HR = 4.76, P < 0.001). Our study revealed the prognostic value of the GI/HRD score in lung adenocarcinoma, but not for all lung cancer. Moreover, the combination of the GI/HRD score and TP53 status could be a promising strategy to predict the prognosis of patients with lung adenocarcinoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
