

Quantification of Low-Attenuation Plaque Burden from Coronary CT Angiography: A Head-to-Head Comparison with Near-Infrared Spectroscopy Intravascular US
- PMID: 37908555
- PMCID: PMC10613924
- DOI: 10.1148/ryct.230090
Quantification of Low-Attenuation Plaque Burden from Coronary CT Angiography: A Head-to-Head Comparison with Near-Infrared Spectroscopy Intravascular US
Abstract
Purpose: To determine the association between low-attenuation plaque (LAP) burden at coronary CT angiography (CCTA) and plaque morphology determined with near-infrared spectroscopy intravascular US (NIRS-IVUS) and to compare the discriminative ability for NIRS-IVUS-verified high-risk plaques (HRPs) between LAP burden and visual assessment of LAP.
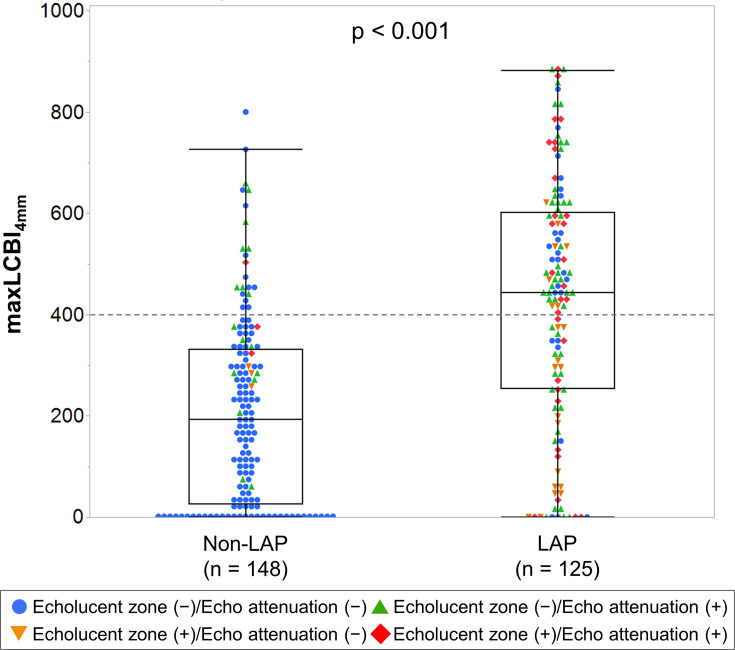
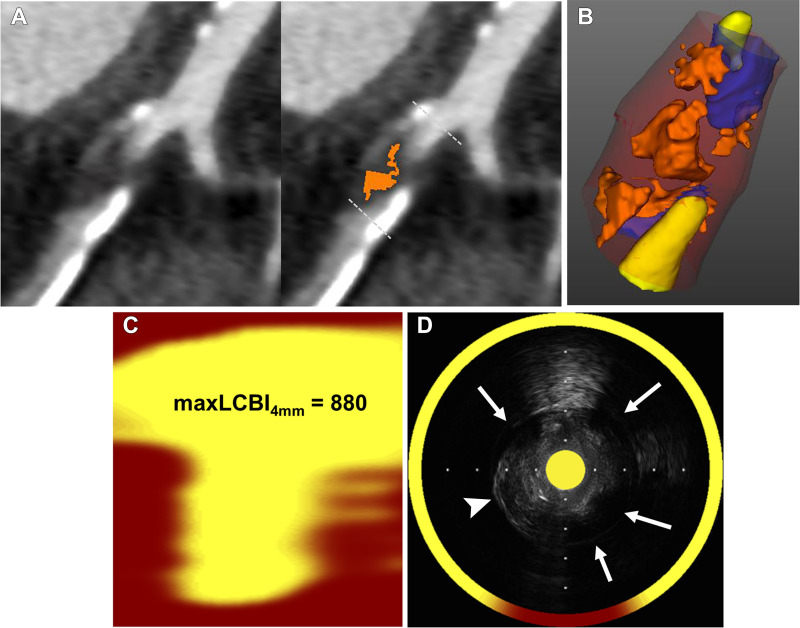
Materials and methods: This Health Insurance Portability and Accountability Act-compliant retrospective study included consecutive patients who underwent CCTA before NIRS-IVUS between October 2019 and October 2022 at two facilities. LAPs were visually identified as having a central focal area of less than 30 HU using the pixel lens technique. LAP burden was calculated as the volume of voxels with less than 30 HU divided by vessel volume. HRPs were defined as plaques with one of the following NIRS-IVUS-derived high-risk features: maximum 4-mm lipid core burden index greater than 400 (lipid-rich plaque), an echolucent zone (intraplaque hemorrhage), or echo attenuation (cholesterol clefts). Multivariable analysis was performed to evaluate NIRS-IVUS-derived parameters associated with LAP burden. The discriminative ability for NIRS-IVUS-verified HRPs was compared using receiver operating characteristic analysis.
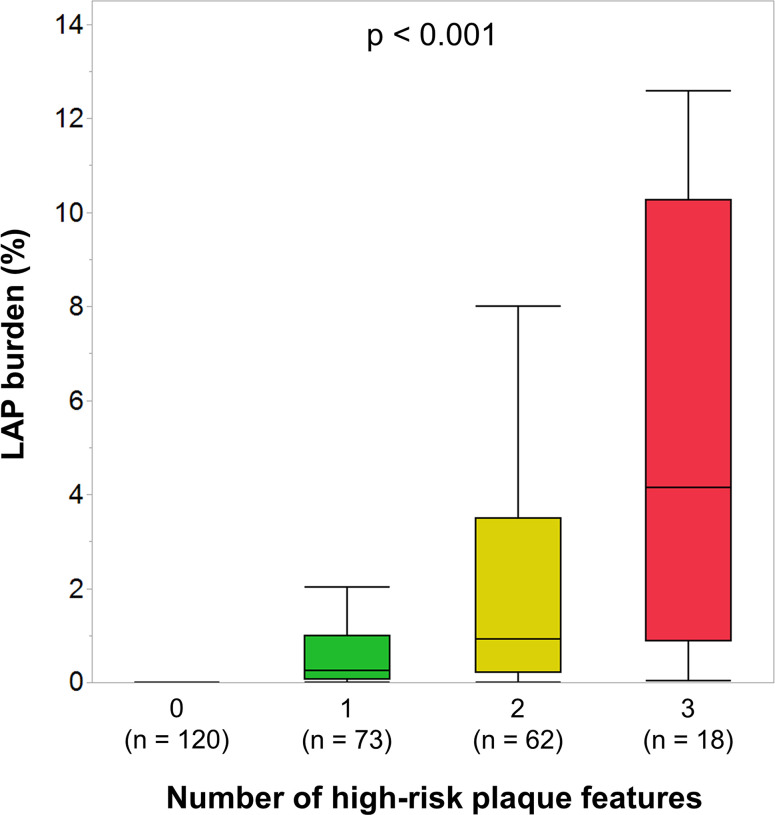
Results: In total, 273 plaques in 141 patients (median age, 72 years; IQR, 63-78 years; 106 males) were analyzed. All the NIRS-IVUS-derived high-risk features were independently linked to LAP burden (P < .01 for all). LAP burden increased with the number of high-risk features (P < .001) and had better discriminative ability for HRPs than plaque attenuation by visual assessment (area under the receiver operating characteristic curve, 0.93 vs 0.89; P = .02).
Conclusion: Quantification of LAP burden improved HRP assessment compared with visual assessment. LAP burden was associated with the accumulation of HRP morphology.Keywords: Coronary CT Angiography, Intraplaque Hemorrhage, Lipid-Rich Plaque, Low Attenuation Plaque, Near-Infrared Spectroscopy Intravascular Ultrasound Supplemental material is available for this article. See also the commentary by Ferencik in this issue.© RSNA, 2023.
Keywords: Coronary CT Angiography; Intraplaque Hemorrhage; Lipid-Rich Plaque; Low Attenuation Plaque; Near-Infrared Spectroscopy Intravascular Ultrasound.
© 2023 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of conflicts of interest: H.T. No relevant relationships. H.M. No relevant relationships. S.C. No relevant relationships. S.H. No relevant relationships. H.O. No relevant relationships. K.I. No relevant relationships. D.I. No relevant relationships. K.K. No relevant relationships. A.S. No relevant relationships. T.H. No relevant relationships. Y.O. No relevant relationships. R.K. No relevant relationships. P.J.S. Grant to author's institution from Siemens Healthcare; NIH grants; software licenses from Cedars-Sinai; consulting fees from Synektik; JNC associate editor; president, Society of Nuclear Medicine & Molecular Imaging Cardiovascular Council. D.D. Royalties/licenses from Cedars-Sinai Medical Center; patents issued (US8885905B2). T.S. No relevant relationships.
Figures




References
-
- Maurovich-Horvat P , Ferencik M , Voros S , Merkely B , Hoffmann U . Comprehensive plaque assessment by coronary CT angiography . Nat Rev Cardiol 2014. ; 11 ( 7 ): 390 – 402 . - PubMed
-
- Shaw LJ , Blankstein R , Bax JJ , et al. . Society of Cardiovascular Computed Tomography / North American Society of Cardiovascular Imaging - expert consensus document on coronary CT imaging of atherosclerotic plaque . J Cardiovasc Comput Tomogr 2021. ; 15 ( 2 ): 93 – 109 . - PubMed
-
- Motoyama S , Sarai M , Harigaya H , et al. . Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome . J Am Coll Cardiol 2009. ; 54 ( 1 ): 49 – 57 . - PubMed
-
- Maroules CD , Hamilton-Craig C , Branch K , et al. . Coronary artery disease reporting and data system (CAD-RADS™): Inter-observer agreement for assessment categories and modifiers . J Cardiovasc Comput Tomogr 2018. ; 12 ( 2 ): 125 – 130 . - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
