

Influenza vaccination in Western Australian children: Exploring the health benefits and cost savings of increased vaccine coverage in children
- PMID: 37908895
- PMCID: PMC10613898
- DOI: 10.1016/j.jvacx.2023.100399
Influenza vaccination in Western Australian children: Exploring the health benefits and cost savings of increased vaccine coverage in children
Abstract
Introduction: To assess potential benefits and direct healthcare cost savings with expansion of an existing childhood influenza immunisation program, we developed a dynamic transmission model for the state of Western Australia, evaluating increasing coverage in children < 5 years and routinely immunising school-aged children.
Methods: A deterministic compartmental Susceptible-Exposed-Infectious-Recovered age-stratified transmission model was developed and calibrated using laboratory-notification and hospitalisation data. Base case vaccine coverage estimates were derived from 2019 data and tested under moderate, low and high vaccine effectiveness settings. The impact of increased coverage on the burden of influenza, influenza-associated presentations and net costs were assessed using the transmission model and estimated health utilisation costs.
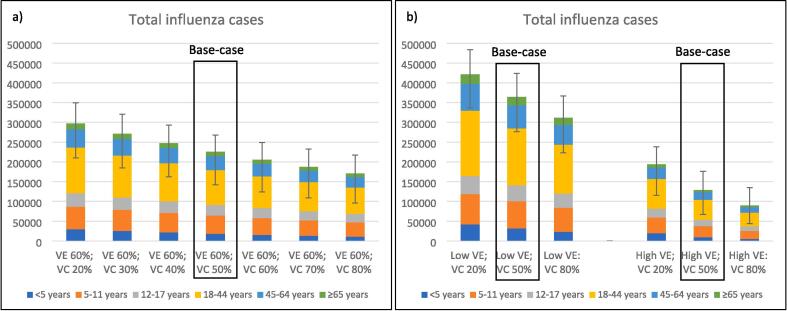
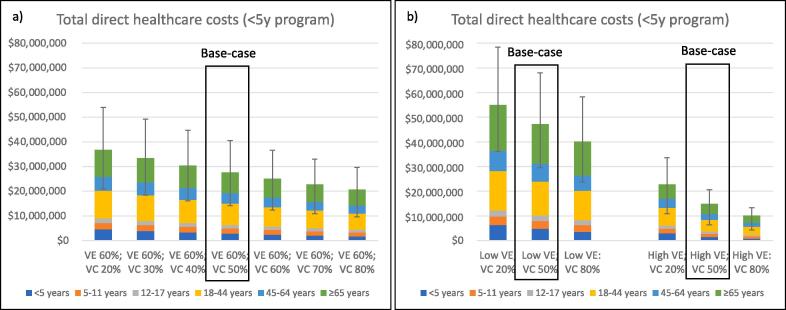
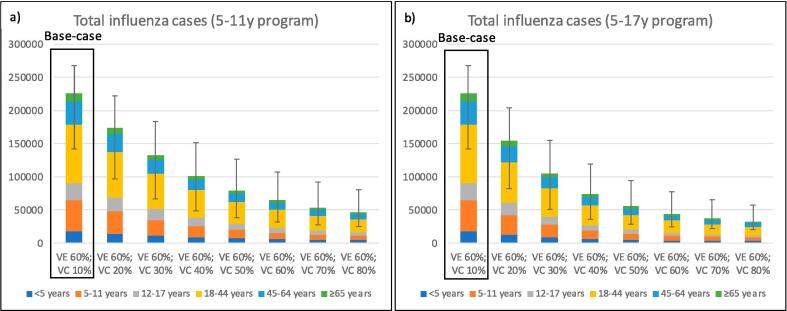
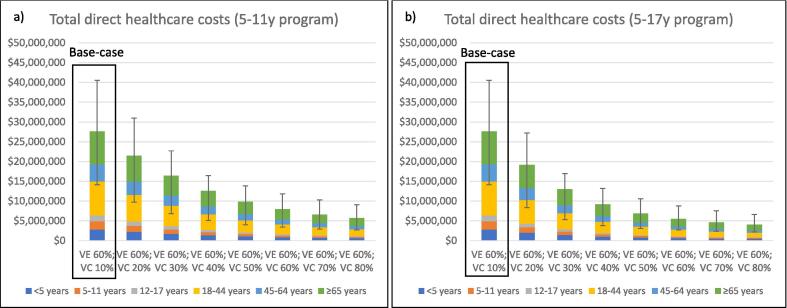
Results: Under base case vaccine coverage and moderate vaccine effectiveness settings, 225,460 influenza cases are expected annually across all ages. Direct healthcare costs of influenza were estimated to be A$27,608,286 per annum, dominated by hospital costs. Net cost savings of >$A1.5 million dollars were observed for every 10 % increase in vaccine coverage in children < 5 years. Additional benefits were observed by including primary school age children (5-11 years) in the funded influenza vaccination program - a reduction in cases, presentations, hospitalisations and approximately $A4 million net costs savings were observed for every 10 % increase in coverage. The further addition of older children (12-17 years) resulted in only moderate additional net cost savings figures, compared with a 5-11year-old program alone. Net costs savings were predominantly derived by a reduction in influenza-associated hospitalisation in adults.
Conclusions: Any increase in influenza vaccine coverage in children < 5 years, above a base case of 50 % coverage resulted in a substantive reduction in influenza cases, presentations, hospitalisations and net costs when applied to the West Australian population. However, the most impactful pediatric program, from both a disease prevention and costs perspective, would be one that increased vaccination coverage among primary-school aged children.
Keywords: Child; Costs; Influenza; Influenza vaccination.
© 2023 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Cost-utility analysis of increasing uptake of universal seasonal quadrivalent influenza vaccine (QIV) in children aged 6 months and older in Germany.Hum Vaccin Immunother. 2022 Nov 30;18(5):2058304. doi: 10.1080/21645515.2022.2058304. Epub 2022 Apr 29. Hum Vaccin Immunother. 2022. PMID: 35486410 Free PMC article.
-
Cost-benefit analysis of a national influenza vaccination program in preventing hospitalisation costs in Australian adults aged 50-64 years old.Vaccine. 2019 Sep 20;37(40):5979-5985. doi: 10.1016/j.vaccine.2019.08.028. Epub 2019 Aug 28. Vaccine. 2019. PMID: 31473001
-
Vaccination of children with a live-attenuated, intranasal influenza vaccine - analysis and evaluation through a Health Technology Assessment.GMS Health Technol Assess. 2014 Oct 30;10:Doc03. doi: 10.3205/hta000119. eCollection 2014. GMS Health Technol Assess. 2014. PMID: 25371764 Free PMC article.
-
[A full economic evaluation of extensive vaccination against rotavirus with RIX4414 vaccine at National and Regional level in Italy].Ann Ig. 2013 Jan-Feb;25(1):43-56. doi: 10.7416/ai.2013.1905. Ann Ig. 2013. PMID: 23435779 Italian.
-
Influenza Vaccination: Effectiveness, Indications, and Limits in the Pediatric Population.Front Pediatr. 2019 Jul 30;7:317. doi: 10.3389/fped.2019.00317. eCollection 2019. Front Pediatr. 2019. PMID: 31417886 Free PMC article. Review.
References
-
- Ozawa S., Clark S., Portnoy A., Grewal S., Brenzel L., Walker D.G. Return on investment from childhood immunization in low- and middle-income countries, 2011–20. Health Aff (Millwood) 2016;35(2):199–207. - PubMed
-
- National Notifiable Diseases Surveillance System (NNDSS) public dataset. National Notifiable Diseases Surveillance System (NNDSS) public dataset – influenza (laboratory confirmed). In: Department of Health and Aged Care, editor. https://www.health.gov.au/resources/collections/nndss-public-datasets (accessed 11th January 2023): Australian Government; 2022.
-
- Blyth C.C., Macartney K.K., Hewagama S., Senenayake S., Friedman N.D., Simpson G., et al. Influenza epidemiology, vaccine coverage and vaccine effectiveness in children admitted to sentinel Australian hospitals in 2014: the Influenza Complications Alert Network (FluCAN) Euro Surveill. 2016;21(30) - PubMed
-
- Blyth C.C., Macartney K.K., McRae J., Clark J.E., Marshall H.S., Buttery J., et al. Influenza Epidemiology, Vaccine Coverage and Vaccine Effectiveness in Children Admitted to Sentinel Australian Hospitals in 2017: Results from the PAEDS-FluCAN Collaboration. Clin Infect Dis. 2019;68(6):940–948. - PubMed
LinkOut - more resources
Full Text Sources
