

Association of Somatic TET2 Mutations With Giant Cell Arteritis
- PMID: 37909388
- PMCID: PMC10922498
- DOI: 10.1002/art.42738
Association of Somatic TET2 Mutations With Giant Cell Arteritis
Abstract
Objective: Giant cell arteritis (GCA) is an age-related vasculitis. Prior studies have identified an association between GCA and hematologic malignancies (HMs). How the presence of somatic mutations that drive the development of HMs, or clonal hematopoiesis (CH), may influence clinical outcomes in GCA is not well understood.
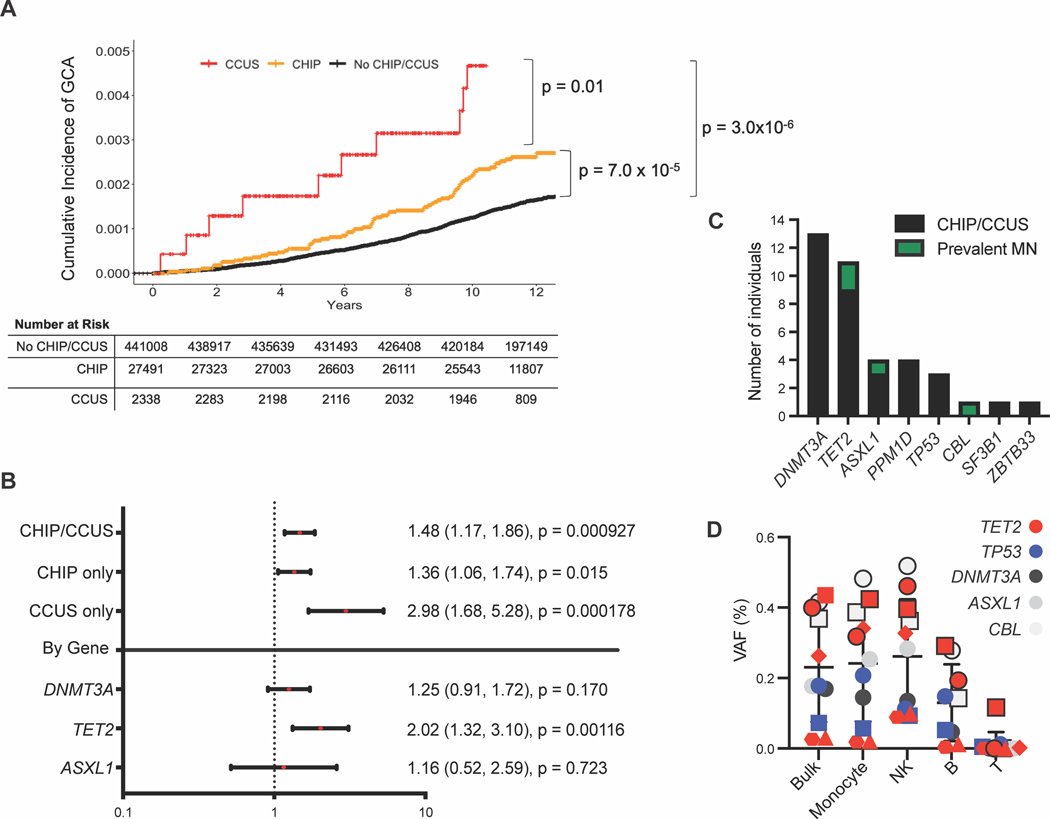
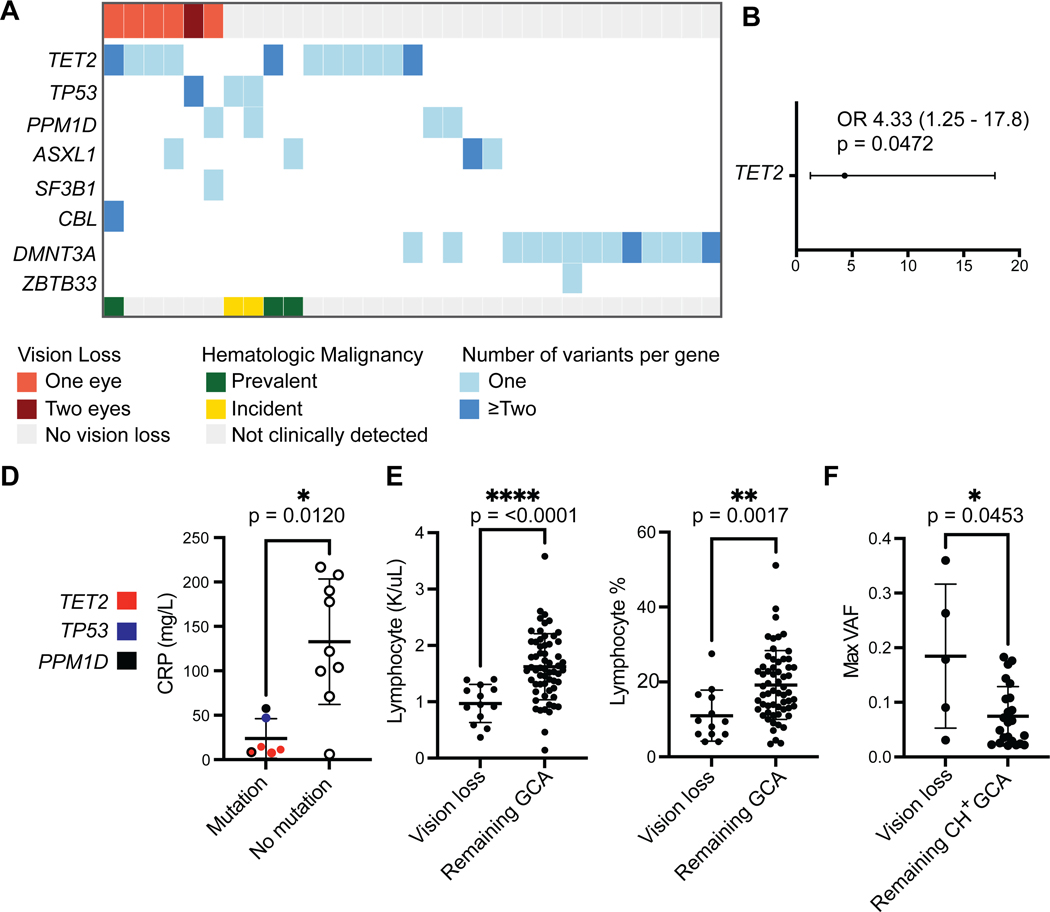
Methods: To examine an association between CH and GCA, we analyzed sequenced exomes of 470,960 UK Biobank (UKB) participants for the presence of CH and used multivariable Cox regression. To examine the clinical phenotype of GCA in patients with and without somatic mutations across the spectrum of CH to HM, we performed targeted sequencing of blood samples and electronic health record review on 114 patients with GCA seen at our institution. We then examined associations between specific clonal mutations and GCA disease manifestations.
Results: UKB participants with CH had a 1.48-fold increased risk of incident GCA compared to UKB participants without CH. GCA risk was highest among individuals with cytopenia (hazard ratio [HR] 2.98, P = 0.00178) and with TET2 mutation (HR 2.02, P = 0.00116). Mutations were detected in 27.2% of our institutional GCA cohort, three of whom had HM at GCA diagnosis. TET2 mutations were associated with vision loss in patients with GCA (odds ratio 4.33, P = 0.047).
Conclusions: CH increases risk for development of GCA in a genotype-specific manner, with the greatest risk being conferred by the presence of mutations in TET2. Somatic TET2 mutations likewise increase the risk of GCA-associated vision loss. Integration of somatic genetic testing in GCA diagnostics may be warranted in the future.
© 2023 The Authors. Arthritis & Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures
References
-
- Roupie AL, et al., Vasculitis associated with myelodysplastic syndrome and chronic myelomonocytic leukemia: French multicenter case-control study. Semin Arthritis Rheum, 2020. 50(5): p. 879–884. - PubMed
-
- Mekinian A, et al., Systemic inflammatory and autoimmune manifestations associated with myelodysplastic syndromes and chronic myelomonocytic leukaemia: a French multicentre retrospective study. Rheumatology (Oxford), 2016. 55(2): p. 291–300. - PubMed
MeSH terms
Substances
Grants and funding
- P01-CA-108631/AR/NIAMS NIH HHS/United States
- R01 HL082945/HL/NHLBI NIH HHS/United States
- P30 AR070253/AR/NIAMS NIH HHS/United States
- 5T32HL007604-37/AR/NIAMS NIH HHS/United States
- P30-AR070253/AR/NIAMS NIH HHS/United States
- K99 HG012956/HG/NHGRI NIH HHS/United States
- R43 AR055855/AR/NIAMS NIH HHS/United States
- R01-HL-082945/AR/NIAMS NIH HHS/United States
- K08 CA263555/CA/NCI NIH HHS/United States
- R01-HL-148050/AR/NIAMS NIH HHS/United States
- R35 CA253125/CA/NCI NIH HHS/United States
- T32HL116324/AR/NIAMS NIH HHS/United States
- P50 CA206963/CA/NCI NIH HHS/United States
- T32-AR-055855/AR/NIAMS NIH HHS/United States
- T32 HL116324/HL/NHLBI NIH HHS/United States
- P01 CA066996/CA/NCI NIH HHS/United States
- K08-AR072791/AR/NIAMS NIH HHS/United States
- HHMI/Howard Hughes Medical Institute/United States
- K07-CA-263555/AR/NIAMS NIH HHS/United States
- K08 AR072791/AR/NIAMS NIH HHS/United States
- P01 CA108631/CA/NCI NIH HHS/United States
- DDCF/Doris Duke Charitable Foundation/United States
- R01 HL148050/HL/NHLBI NIH HHS/United States
- T32 HL007604/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
