

Demographics and Clinical Characteristics Associated with the Spread of New-Onset Laryngeal Dystonia
- PMID: 37909788
- PMCID: PMC11157453
- DOI: 10.1002/lary.31146
Demographics and Clinical Characteristics Associated with the Spread of New-Onset Laryngeal Dystonia
Abstract
Objectives: Adult-onset idiopathic laryngeal dystonia (LD) can be associated with the risk of spread to muscles in the body. Subjects with extralaryngeal onset of dystonia have exhibited spread to the larynx. Previous studies analyze the spread of other dystonias but emphasis has not been placed on LD. The objective was to identify demographic and clinical factors contributing to the spread of dystonia to and from the larynx.
Methods: Data were obtained from the Dystonia Coalition (DC)-patients from 49 international clinical centers. Clinical and demographic data was taken from 143 out of 409 patients with diagnosed LD. Patient criteria included adult-onset LD diagnosed on exam with no co-morbid neurologic conditions and no dystonia in other locations.
Results: Among the 143 patients, 94 (65.7%) patients were diagnosed with focal laryngeal onset, with the remainder having extralaryngeal onset. Family history and age at study were statistically significant indicators of a patient developing laryngeal versus extralaryngeal onset of dystonia. Among the laryngeal onset group, 21 cases (22.3%) had an average time of 5.81 ± 5.79 years to spread from diagnosis, most commonly to neck (61.9%). Among extralaryngeal onset patients, mean time of larynx spread was 7.92 ± 7.737 years, most commonly to neck (22.7%).
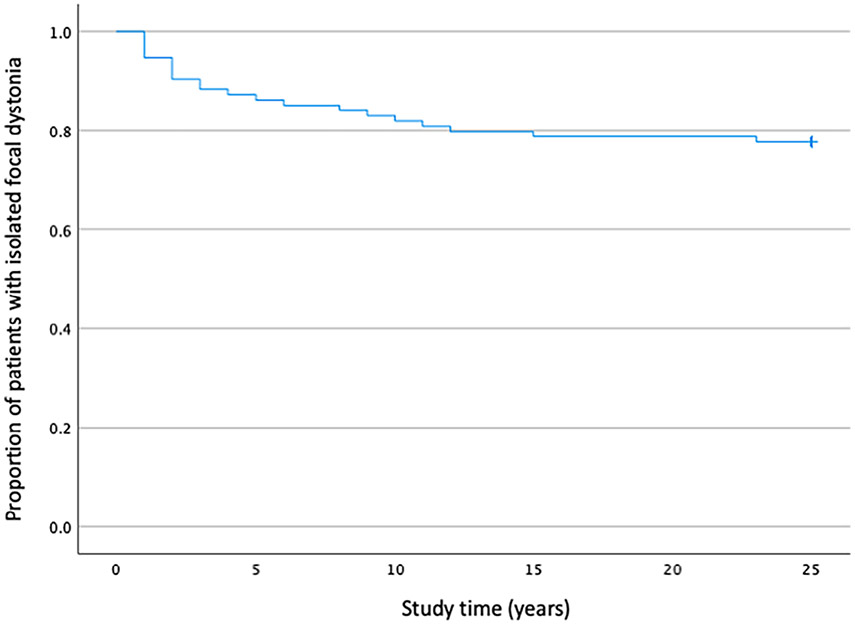
Conclusions: Our data indicates approximately a quarter of patients with laryngeal-onset dystonia will exhibit spread. There were no demographic or clinical factors that were statistically predictive of the likelihood of spread from larynx. Patients with dystonia elsewhere in the body should be counseled on the possibility of spread to larynx, and vice versa.
Level of evidence: 4 Laryngoscope, 134:2295-2299, 2024.
Keywords: dystonia; laryngeal dystonia; larynx.
© 2023 The Authors. The Laryngoscope published by Wiley Periodicals LLC on behalf of The American Laryngological, Rhinological and Otological Society, Inc.
Conflict of interest statement
The authors have no financial relationships or conflicts of interest to disclose.
Figures
Similar articles
-
Spread of dystonia in patients with idiopathic adult-onset laryngeal dystonia.Eur J Neurol. 2018 Nov;25(11):1341-1344. doi: 10.1111/ene.13731. Epub 2018 Jul 31. Eur J Neurol. 2018. PMID: 29935029
-
Incidence and risk factors for secondary extralaryngeal dystonia in patients with laryngeal dystonia.Am J Otolaryngol. 2024 Jan-Feb;45(1):104090. doi: 10.1016/j.amjoto.2023.104090. Epub 2023 Oct 12. Am J Otolaryngol. 2024. PMID: 37865985
-
Risk of spread in adult-onset isolated focal dystonia: a prospective international cohort study.J Neurol Neurosurg Psychiatry. 2020 Mar;91(3):314-320. doi: 10.1136/jnnp-2019-321794. Epub 2019 Dec 17. J Neurol Neurosurg Psychiatry. 2020. PMID: 31848221 Free PMC article.
-
Do primary adult-onset focal dystonias share aetiological factors?Brain. 2007 May;130(Pt 5):1183-93. doi: 10.1093/brain/awl355. Epub 2007 Jan 22. Brain. 2007. PMID: 17242025 Review.
-
Phenomenology, genetics, and CNS network abnormalities in laryngeal dystonia: A 30-year experience.Laryngoscope. 2018 Jan;128 Suppl 1(Suppl 1):S1-S9. doi: 10.1002/lary.27003. Epub 2017 Dec 8. Laryngoscope. 2018. PMID: 29219190 Free PMC article. Review.
References
-
- Hintze JM, Ludlow CL, Bansberg SF, Adler CH, Lott DG. Spasmodic dysphonia: a review. Part 1: pathogenic factors. Otolaryngol Head Neck Surg. 2017;157(4):551–557. - PubMed
-
- Chhetri DK, Berke GS. Treatment of adductor spasmodic dysphonia with selective laryngeal adductor denervation and reinnervation surgery. Otolaryngol Clin North Am. 2006;39(1):101–109. - PubMed
-
- Weiss EM, Hershey T, Karimi M, et al. Relative risk of spread of symptoms among the focal onset primary dystonias. Mov Disord. 2006;21(8):1175–1181. - PubMed
-
- Svetel M, Pekmezović T, Jović J, et al. Spread of primary dystonia in relation to initially affected region. J Neurol. 2007;254(7):879–883. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
