

Surgical management of metastatic Hürthle cell carcinoma to the skull base, cortex, and spine: illustrative case
- PMID: 37910014
- PMCID: PMC10566523
- DOI: 10.3171/CASE23263
Surgical management of metastatic Hürthle cell carcinoma to the skull base, cortex, and spine: illustrative case
Abstract
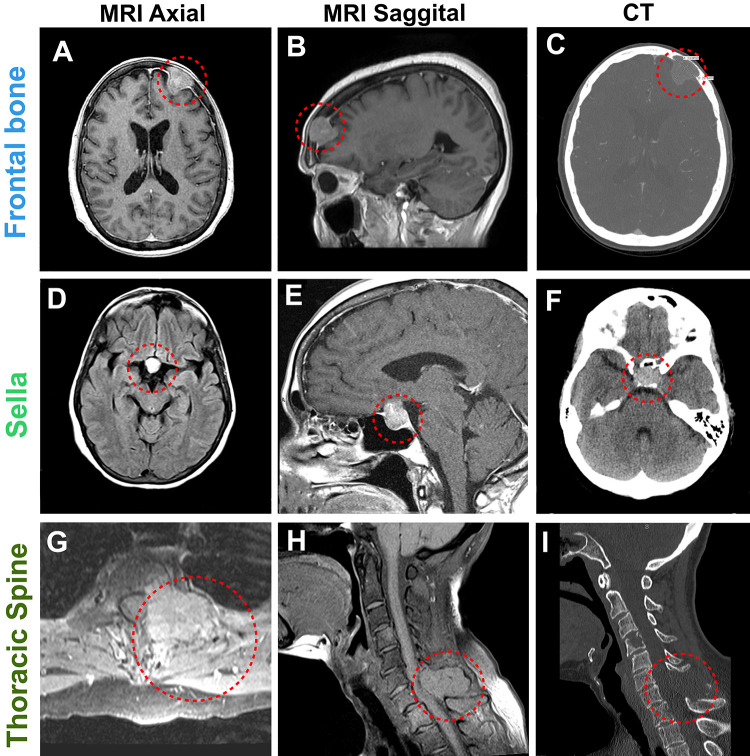
Background: Hürthle cell carcinoma (HCC) is an unusual and aggressive variant of the follicular type of differentiated thyroid cancer (DTC), accounting for less than 3% of DTCs but posing the highest risk of metastasis. Brain metastases are uncommonly reported in the literature but pose a poor prognosis. The low rate of brain metastases from HCC coupled with ambiguous treatment protocols for the extracranial disease complicate successful disease management and definitive treatment strategy. The authors present the case of a patient with HCC metastasis to the skull base, cortex, and spine with recent tibial metastasis.
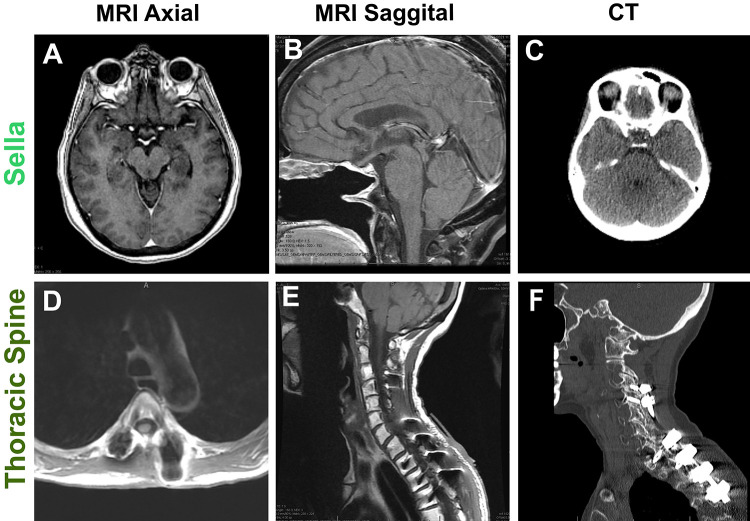
Observations: Despite the presence of metastasis to the cortex, skull base, and spine, the patient responded very well to radiation therapy, sellar mass resection, and cervical spine decompression and fixation and has made a remarkable recovery.
Lessons: The authors' multidisciplinary approach to the patient's care, including a diverse team of specialists from oncology, neurosurgery, orthopedic surgery, radiology, endocrinology, and collaboration with clinical trial researchers, was fundamental to her successful outcome, demonstrating the utility of intersecting specialties in successful outcomes in neuro-oncological patient care.
Keywords: metastatic Hürthle cell carcinoma; multidisciplinary management; neurosurgery.
Conflict of interest statement
Figures
References
-
- Yutan E, Clark OH. Hürthle cell carcinoma. Curr Treat Options Oncol. 2001;2(4):331–335. - PubMed
-
- Mendes VC, Linhares P, Fonseca E, Ribeiro-Silva ML. Giant skull metastasis of Hürthle cell variant of thyroid’s papillary carcinoma. J Neurooncol. 2008;86(3):311–312. - PubMed
-
- Healy AT, Otvos B, Schroeder J, Hamrahian AH, Angelov L, Kamian K. Hurthle cell carcinoma presenting as a single choroid plexus metastasis. J Clin Neurosci. 2014;21(8):1448–1450. - PubMed
LinkOut - more resources
Full Text Sources
