

Fecal microbiota transplantation promotes reduction of antimicrobial resistance by strain replacement
- PMID: 37910603
- PMCID: PMC10821315
- DOI: 10.1126/scitranslmed.abo2750
Fecal microbiota transplantation promotes reduction of antimicrobial resistance by strain replacement
Abstract
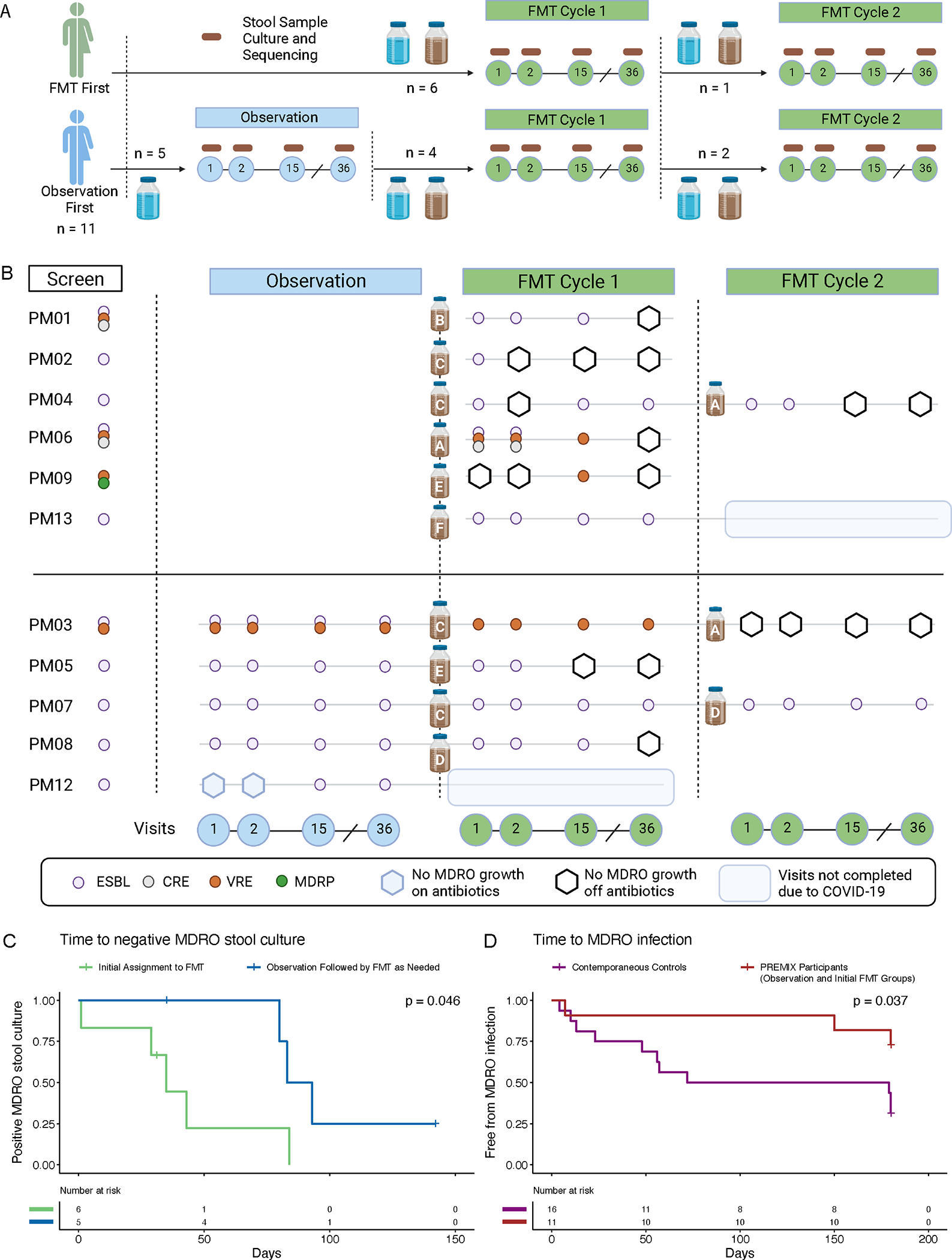
Multidrug-resistant organism (MDRO) colonization is a fundamental challenge in antimicrobial resistance. Limited studies have shown that fecal microbiota transplantation (FMT) can reduce MDRO colonization, but its mechanisms are poorly understood. We conducted a randomized, controlled trial of FMT for MDRO decolonization in renal transplant recipients called PREMIX (NCT02922816). Eleven participants were enrolled and randomized 1:1 to FMT or an observation period followed by delayed FMT if stool cultures were MDRO positive at day 36. Participants who were MDRO positive after one FMT were treated with a second FMT. At last visit, eight of nine patients who completed all treatments were MDRO culture negative. FMT-treated participants had longer time to recurrent MDRO infection versus PREMIX-eligible controls who were not treated with FMT. Key taxa (Akkermansia muciniphila, Alistipes putredinis, Phocaeicola dorei, Phascolarctobacterium faecium, Alistipes species, Mesosutterella massiliensis, Barnesiella intestinihominis, and Faecalibacterium prausnitzii) from the single feces donor used in the study that engrafted in recipients and metabolites such as short-chain fatty acids and bile acids in FMT-responding participants uncovered leads for rational microbiome therapeutic and diagnostic development. Metagenomic analyses revealed a previously unobserved mechanism of MDRO eradication by conspecific strain competition in an FMT-treated subset. Susceptible Enterobacterales strains that replaced baseline extended-spectrum β-lactamase-producing strains were not detectable in donor microbiota manufactured as FMT doses but in one case were detectable in the recipient before FMT. These data suggest that FMT may provide a path to exploit strain competition to reduce MDRO colonization.
Conflict of interest statement
Figures




References
-
- Buelow E, Gonzalez TB, Versluis D, Oostdijk EAN, Ogilvie LA, van Mourik MSM, Oosterink E, van Passel MWJ, Smidt H, D’Andrea MM, de Been M, Jones BV, Willems RJL, Bonten MJM, van Schaik W, Effects of selective digestive decontamination (SDD) on the gut resistome, J. Antimicrob. Chemother. 69, 2215–2223 (2014). - PubMed
-
- Hayden MK, Lin MY, Lolans K, Weiner S, Blom D, Moore NM, Fogg L, Henry D, Lyles R, Thurlow C, Sikka M, Hines D, Weinstein RA, Centers for Disease Control and Prevention Epicenters Program, Prevention of colonization and infection by Klebsiella pneumoniae carbapenemase-producing enterobacteriaceae in long-term acute-care hospitals., Clin. Infect. Dis. 60, 1153–61 (2015). - PMC - PubMed
-
- Huang SS, Septimus E, Kleinman K, Moody J, Hickok J, Heim L, Gombosev A, Avery TR, Haffenreffer K, Shimelman L, Hayden MK, Weinstein RA, Spencer-Smith C, Kaganov RE, Murphy MV, Forehand T, Lankiewicz J, Coady MH, Portillo L, Sarup-Patel J, Jernigan JA, Perlin JB, Platt R, Chlorhexidine versus routine bathing to prevent multidrug-resistant organisms and all-cause bloodstream infections in general medical and surgical units (ABATE Infection trial): a cluster-randomised trial, Lancet 393, 1205–1215 (2019). - PMC - PubMed
-
- Isendahl J, Giske CG, Hammar U, Sparen P, Tegmark Wisell K, Ternhag A, Nauclér P, Temporal Dynamics and Risk Factors for Bloodstream Infection With Extended-spectrum β-Lactamase-producing Bacteria in Previously-colonized Individuals: National Population-based Cohort Study, Clin. Infect. Dis. 68, 641–649 (2019). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
