

Prognostic value of 18F-FDG PET in uterine cervical cancer patients with stage IIICr allocated by imaging
- PMID: 37914892
- PMCID: PMC10620427
- DOI: 10.1038/s41598-023-46261-2
Prognostic value of 18F-FDG PET in uterine cervical cancer patients with stage IIICr allocated by imaging
Abstract
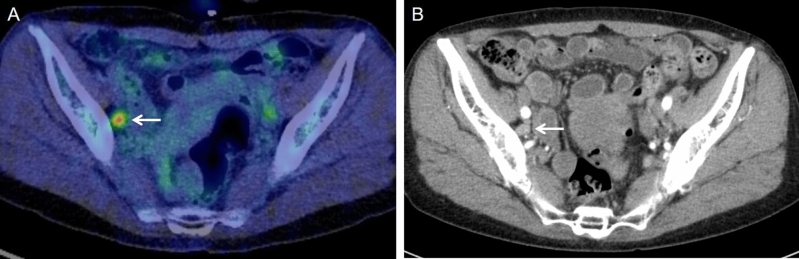
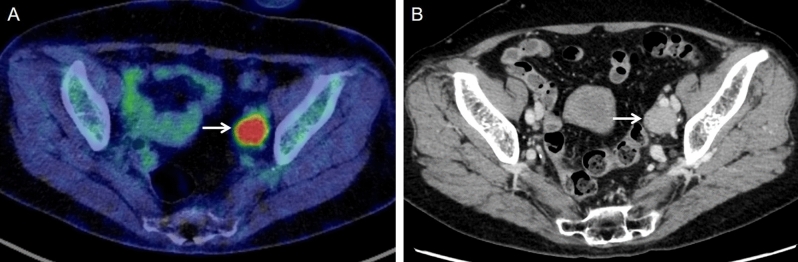
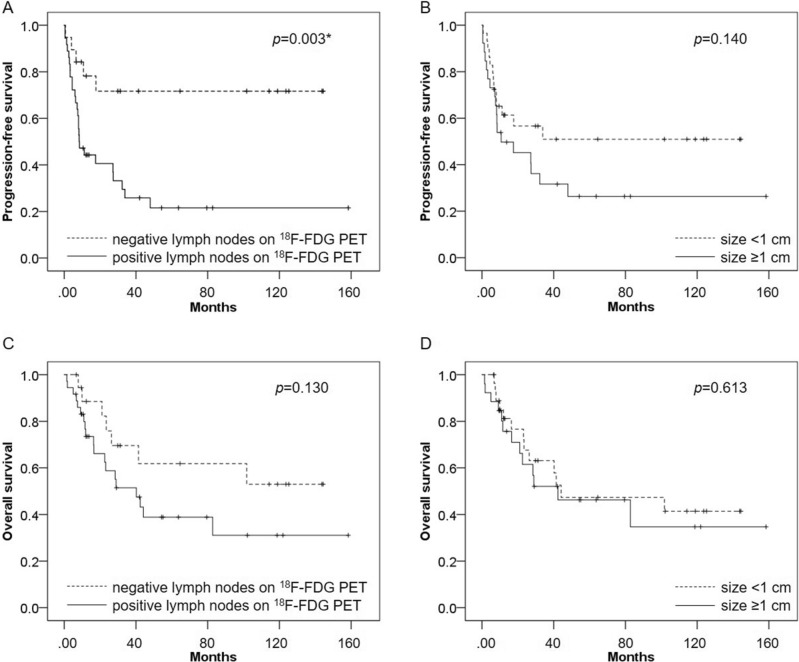
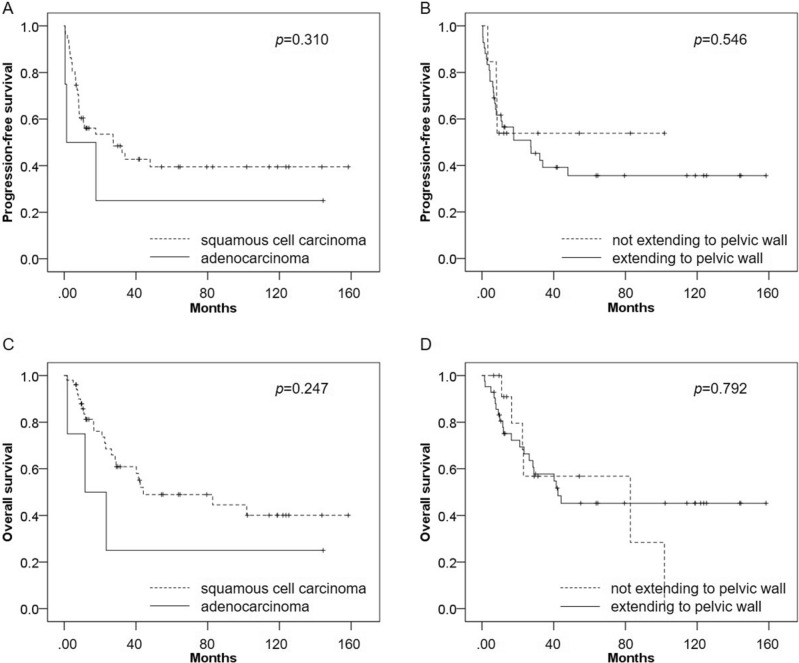
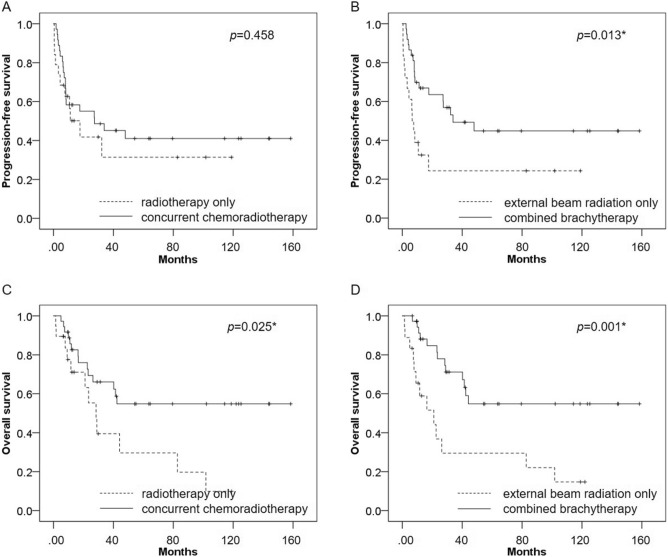
The effect on survival of radiographic lymph node metastasis in uterine cervical cancer patients is more important than before, even though its prognostic value not been well investigated. The aim of our study is to evaluate the prognostic potential of 18F-fluorodeoxyglucose Positron Emission Tomography (18F-FDG PET) compared with Computed Tomography (CT) in uterine cervical cancer patients with stage IIICr allocated by imaging. Fifty-five patients with biopsy-proven primary cervical cancer underwent definitive radiation therapy for stages IIB-IVB of The International Federation of Gynecology and Obstetrics (FIGO) 2018 classifications. The prognostic performance of pretreatment 18F-FDG PET and CT for assessing lymph node metastasis was evaluated by two experienced readers. The PET and CT findings were correlated with the risk of progression-free survival (PFS) and overall survival (OS). Kaplan-Meier survival curves showed that PFS was significantly worse in patients with positive lymph nodes on 18F-FDG PET than in those patients with negative lymph nodes on 18F-FDG PET (p = 0.003), whereas there was no significant difference in PFS between patients with lymph nodes sized ≥ 1 cm and those sized < 1 cm (p = 0.140). Univariate analysis showed that positive lymph nodes on 18F-FDG PET was significantly associated with poor PFS (p = 0.006), whereas lymph node size was not significantly associated with poor PFS (p = 0.145). In multivariate analysis, positive lymph nodes on 18F-FDG PET was significantly associated with poor PFS (p = 0.006) and was an independent prognostic factor for PFS. 18F-FDG PET offers high prognostic value for patients with stage IIICr allocated by imaging compared with CT, suggesting that 18F-FDG PET might be useful in clinical staging decisions and thus promote optimal diagnostic and therapeutic strategies.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Corrigendum to "Revised FIGO staging for carcinoma of the cervix uteri" [Int J Gynecol Obstet 145(2019) 129–135]. Int. J. Gynaecol. Obstet.147, 279–280. 10.1002/ijgo.12969 (2019). - PubMed
