

Prostaglandin and prostaglandin receptors: present and future promising therapeutic targets for pulmonary arterial hypertension
- PMID: 37915044
- PMCID: PMC10619262
- DOI: 10.1186/s12931-023-02559-3
Prostaglandin and prostaglandin receptors: present and future promising therapeutic targets for pulmonary arterial hypertension
Abstract
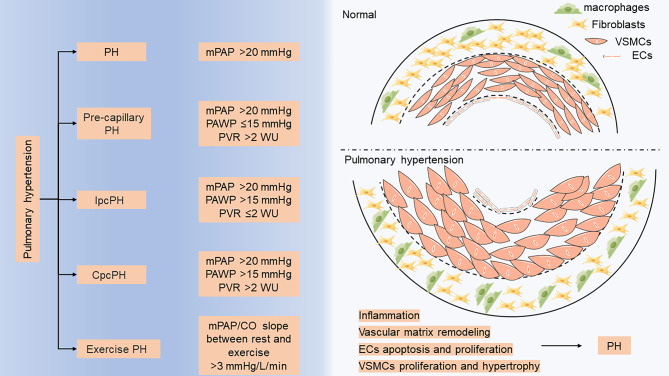
Background: Pulmonary arterial hypertension (PAH), Group 1 pulmonary hypertension (PH), is a type of pulmonary vascular disease characterized by abnormal contraction and remodeling of the pulmonary arterioles, manifested by pulmonary vascular resistance (PVR) and increased pulmonary arterial pressure, eventually leading to right heart failure or even death. The mechanisms involved in this process include inflammation, vascular matrix remodeling, endothelial cell apoptosis and proliferation, vasoconstriction, vascular smooth muscle cell proliferation and hypertrophy. In this study, we review the mechanisms of action of prostaglandins and their receptors in PAH.
Main body: PAH-targeted therapies, such as endothelin receptor antagonists, phosphodiesterase type 5 inhibitors, activators of soluble guanylate cyclase, prostacyclin, and prostacyclin analogs, improve PVR, mean pulmonary arterial pressure, and the six-minute walk distance, cardiac output and exercise capacity and are licensed for patients with PAH; however, they have not been shown to reduce mortality. Current treatments for PAH primarily focus on inhibiting excessive pulmonary vasoconstriction, however, vascular remodeling is recalcitrant to currently available therapies. Lung transplantation remains the definitive treatment for patients with PAH. Therefore, it is imperative to identify novel targets for improving pulmonary vascular remodeling in PAH. Studies have confirmed that prostaglandins and their receptors play important roles in the occurrence and development of PAH through vasoconstriction, vascular smooth muscle cell proliferation and migration, inflammation, and extracellular matrix remodeling.
Conclusion: Prostacyclin and related drugs have been used in the clinical treatment of PAH. Other prostaglandins also have the potential to treat PAH. This review provides ideas for the treatment of PAH and the discovery of new drug targets.
Keywords: Prostaglandin; Prostaglandin receptor; Pulmonary Hypertension.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Sockrider M. What is pulmonary Hypertension? Am J Respir Crit Care Med. 2021;203(5):P12–P3. - PubMed
-
- Hoeper MM, Humbert M, Souza R, Idrees M, Kawut SM, Sliwa-Hahnle K, et al. A global view of pulmonary Hypertension. Lancet Respir Med. 2016;4(4):306–22. - PubMed
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary Hypertension. Eur Heart J. 2022;43(38):3618–731. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
