

Ureteral obstruction may activate kidney latent tuberculosis. A qualitative study
- PMID: 37915382
- PMCID: PMC10616550
- DOI: 10.1016/j.jctube.2023.100402
Ureteral obstruction may activate kidney latent tuberculosis. A qualitative study
Abstract
Objectives: To analyze the hypothesis that ureteral obstruction may activate kidney latent tuberculous though qualitative study of Urogenital Tuberculosis patients.
Methods: A qualitative study was conducted using semistructured interviews in eight patients with Urogenital Tuberculosis. The progression of the disease from the initial symptoms was characterized through the analysis of the clinical and radiological data. The presence of ureteral obstruction prior to the onset of renal tuberculosis was observed in three patients.
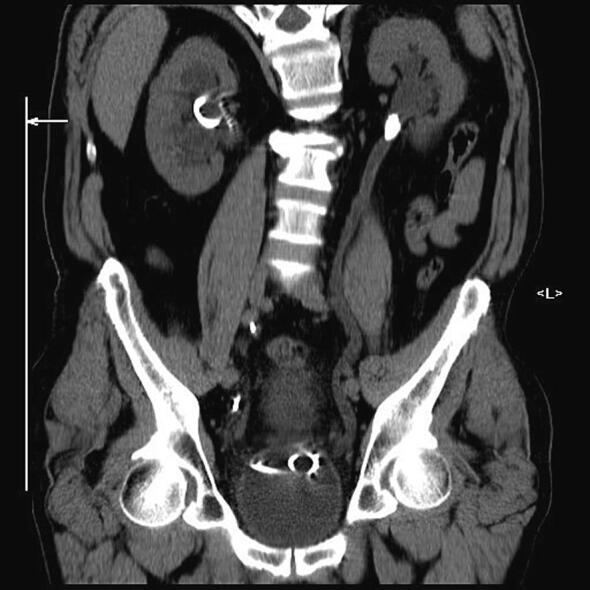
Results: Patient 1: A 58-year-old female had five episodes of acute left ureteral lithiasis in two years prior to left kidney tuberculosis. Patient 2: A 55-year-old male patient had a 1.2 cm proximal left ureteral stone and in the following six months, the diagnosis of tuberculosis was made in a nonfunctioning left kidney with ureteral thickening and stenosis. Patient 3: A 47-year-old male patient had a 1.2 cm stone in the proximal right ureter and developed urinary tuberculosis with a nonfunctioning right kidney and a contracted bladder.
Conclusion: Kidney tuberculosis may appear in the same kidney that had previously suffered stone ureteral obstruction, which may have created local conditions for the activation of latent foci of renal tuberculosis.
Keywords: Kidney tuberculosis; Tuberculosis; Tuberculosis reactivation; Urinary lithiasis; Urogenital tuberculosis.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures












References
-
- Federmann M., Kley H.K. Miliary tuberculosis after extracorporeal shock-wave lithotripsy. N Engl J Med. 1990;323(17):1212. - PubMed
-
- Yekanath H., Gross P.A., Vitenson J.H. Miliary tuberculosis following ureteral catheterization. Urology. 1980;16(2):197–198. - PubMed
-
- Shah H., Dnb M., Shah H.N., Chibber P.J. Renal tuberculosis simulating xanthogranulomatous pyelonephritis with contagious hepatic involvement. Int J Urol. 2006;13 - PubMed
-
- Tong A., Sainsbury P., Craig J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. - PubMed
LinkOut - more resources
Full Text Sources
