

Feasibility of gray-blood late gadolinium enhancement evaluation in young patients with congenital and acquired heart disease
- PMID: 37915741
- PMCID: PMC10616296
- DOI: 10.3389/fcvm.2023.1269412
Feasibility of gray-blood late gadolinium enhancement evaluation in young patients with congenital and acquired heart disease
Abstract
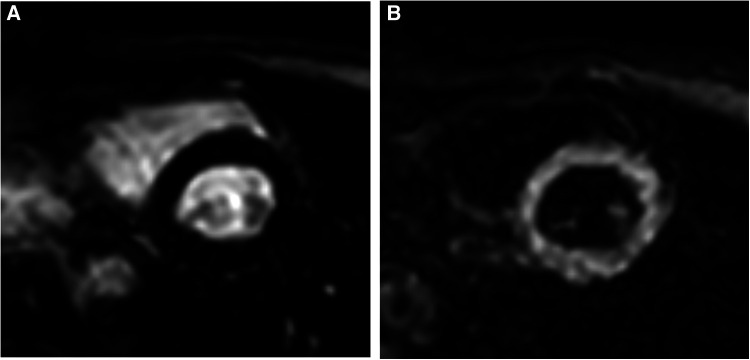
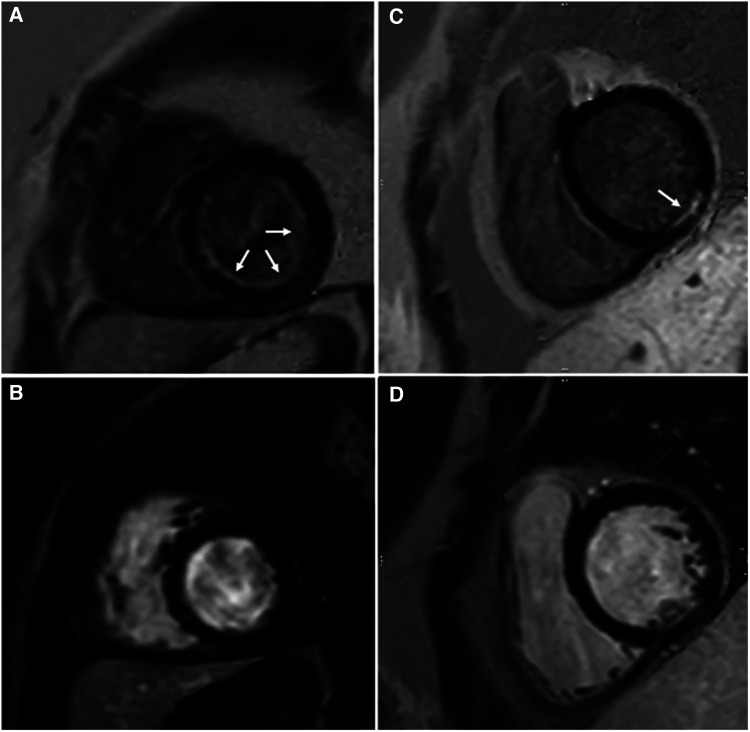
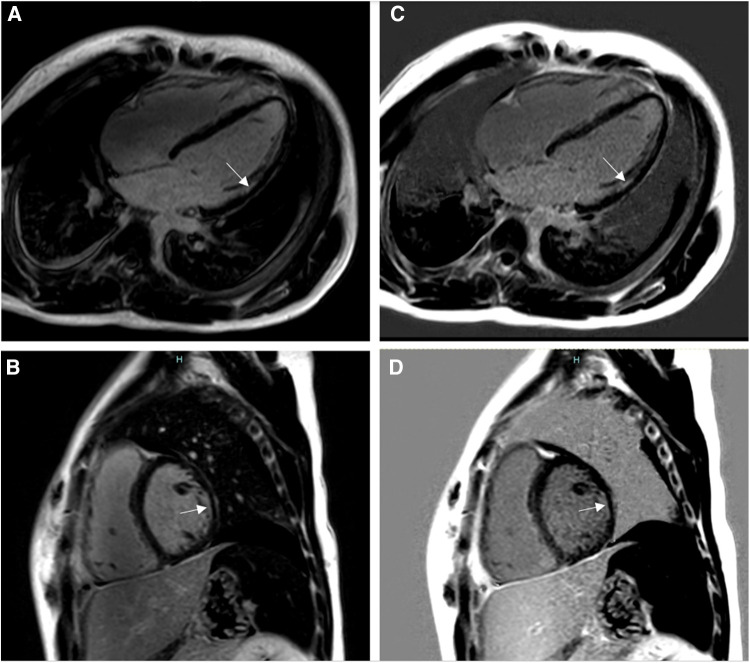
Background: Late gadolinium enhancement (LGE) sequences have become common in pediatric cardiovascular magnetic resonance (CMR) to assess for myocardial fibrosis. Bright-blood late gadolinium enhancement (BB-LGE) by conventional phase-sensitive inversion recovery (PSIR) is commonly utilized, but similar inversion time (TI) value of fibrosis and left ventricular (LV) blood pool can make subendocardial areas difficult to assess. A gray-blood LGE (GB-LGE) technique has been described, targeting nulling of the LV blood pool and demonstrating improvement in ischemic scar detection over BB-LGE in adult patients. We sought to evaluate the feasibility of the GB-LGE technique in a young population with congenital and acquired heart disease and compare its ability to detect subendocardial scar to conventional BB-LGE.
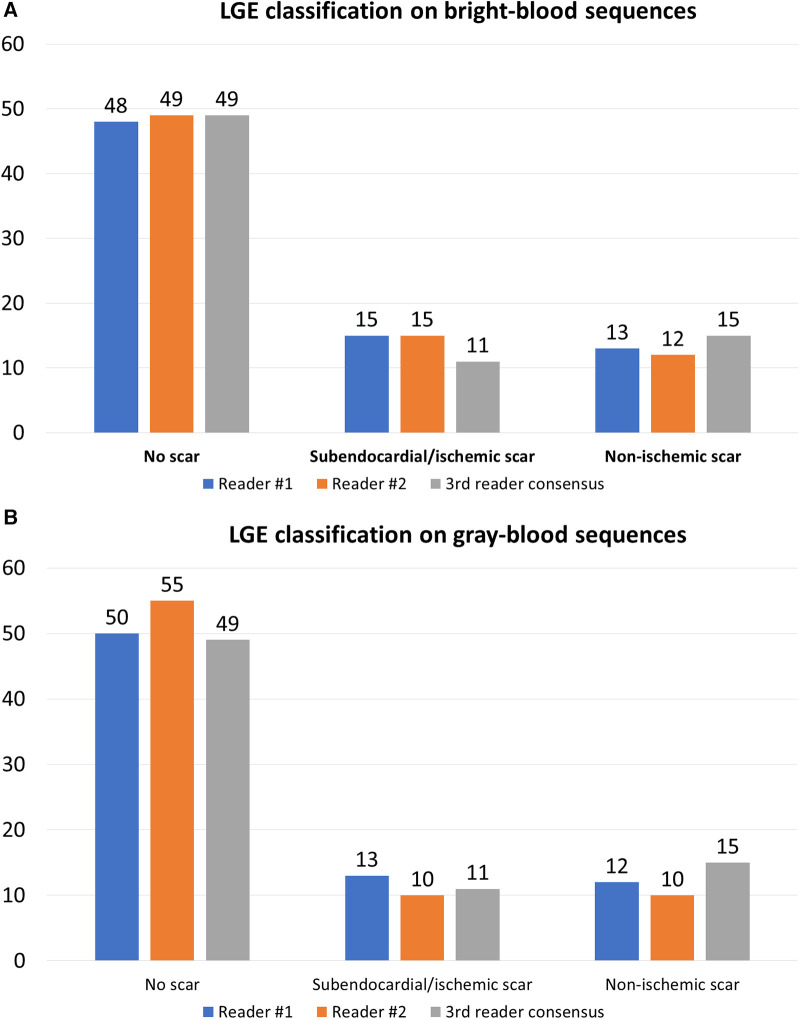
Methods: Seventy-six consecutive patients referred for clinical CMR underwent both BB-LGE and GB-LGE on 1.5 T and 3 T scanners. Conventional PSIR sequences were obtained with TI to null the myocardium (BB-LGE) in short-axis and horizontal long-axis stacks. Same PSIR stacks were immediately repeated with TI to null the blood pool (GB-LGE). Both sequences were reviewed separately a week apart by two readers, blinded to the initial clinical interpretation. Studies were analyzed for overall image quality, confidence in scar detection, confidence in detection of LGE, LGE class, inter- and intra-observer agreement for the presence of scar, and intraclass correlation coefficient (ICC) for total scar burden.
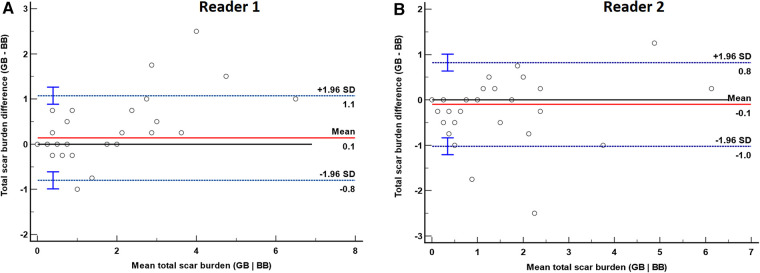
Results: Overall confidence in myocardial scar detection by BB-LGE or GB-LGE as well as grading of image quality were not statistically different [(p = 1 and p = 1) and (p = 0.53, p = 0.18), respectively]. There was very good inter-observer agreement for the presence of scar on BB-LGE (K = 0.88, 95% CI 0.77-0.99) and GB-LGE (K = 0.84, 95% CI 0.7-0.96), as well as excellent intra-observer agreement for both readers (K = 0.93, 95% CI 0.87-0.99; and K = 0.81, 95% CI 0.69-0.95). Interclass correlation coefficient for total scar burden was excellent for BB-LGE (ICC = 0.98, 95% CI 0.96-0.99) and GB-LGE (ICC = 0.94, 95% CI 0.91-0.97).
Conclusions: The GB-LGE technique is feasible in the pediatric population with congenital and acquired heart disease. It can detect subendocardial/ischemic scar similar to conventional bright-blood PSIR sequences in the pediatric population.
Keywords: cardiovascular magnetic resonance; congenital heart disease; late gadolinium enhancement; myocardial fibrosis; phase-sensitive inversion recovery; subendocardial fibrosis.
© 2023 Gonzalez de Alba, Moghari, Browne, Friesen, Fonseca and Malone.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical value of dark-blood late gadolinium enhancement cardiovascular magnetic resonance without additional magnetization preparation.J Cardiovasc Magn Reson. 2019 Jul 29;21(1):44. doi: 10.1186/s12968-019-0556-1. J Cardiovasc Magn Reson. 2019. PMID: 31352900 Free PMC article.
-
Bright-blood and dark-blood phase sensitive inversion recovery late gadolinium enhancement and T1 and T2 maps in a single free-breathing scan: an all-in-one approach.J Cardiovasc Magn Reson. 2021 Nov 8;23(1):126. doi: 10.1186/s12968-021-00823-3. J Cardiovasc Magn Reson. 2021. PMID: 34743718 Free PMC article.
-
Gray blood late gadolinium enhancement cardiovascular magnetic resonance for improved detection of myocardial scar.J Cardiovasc Magn Reson. 2018 Mar 22;20(1):22. doi: 10.1186/s12968-018-0442-2. J Cardiovasc Magn Reson. 2018. PMID: 29562921 Free PMC article.
-
Dark-blood late gadolinium enhancement cardiovascular magnetic resonance for improved detection of subendocardial scar: a review of current techniques.J Cardiovasc Magn Reson. 2021 Jul 22;23(1):96. doi: 10.1186/s12968-021-00777-6. J Cardiovasc Magn Reson. 2021. PMID: 34289866 Free PMC article. Review.
-
Whole-Heart High-Resolution Late Gadolinium Enhancement: Techniques and Clinical Applications.J Magn Reson Imaging. 2022 Apr;55(4):967-987. doi: 10.1002/jmri.27732. Epub 2021 Jun 21. J Magn Reson Imaging. 2022. PMID: 34155715 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources