

Genetic testing in focal segmental glomerulosclerosis: in whom and when?
- PMID: 37915894
- PMCID: PMC10616495
- DOI: 10.1093/ckj/sfad193
Genetic testing in focal segmental glomerulosclerosis: in whom and when?
Abstract
Background: Genetic causes are increasingly recognized in patients with focal segmental glomerulosclerosis (FSGS), but it remains unclear which patients should undergo genetic study. Our objective was to determine the frequency and distribution of genetic variants in steroid-resistant nephrotic syndrome FSGS (SRNS-FSGS) and in FSGS of undetermined cause (FSGS-UC).
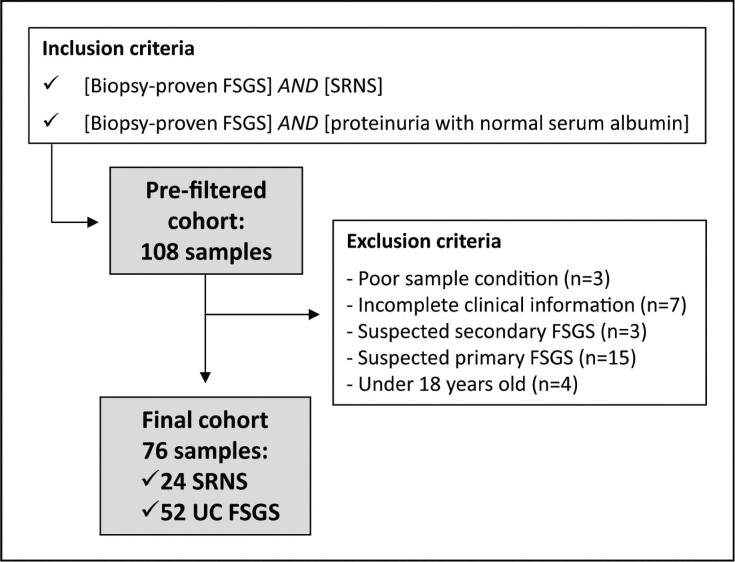
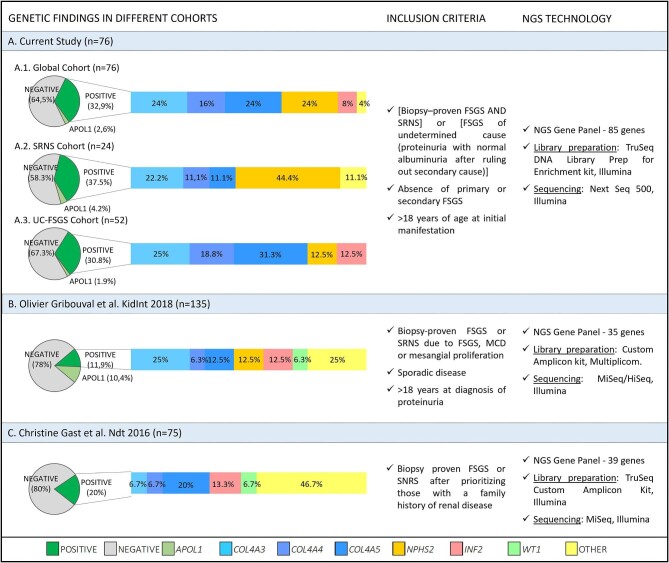
Methods: We performed targeted exome sequencing of 84 genes associated with glomerulopathy in patients with adult-onset SRNS-FSGS or FSGS-UC after ruling out secondary causes.
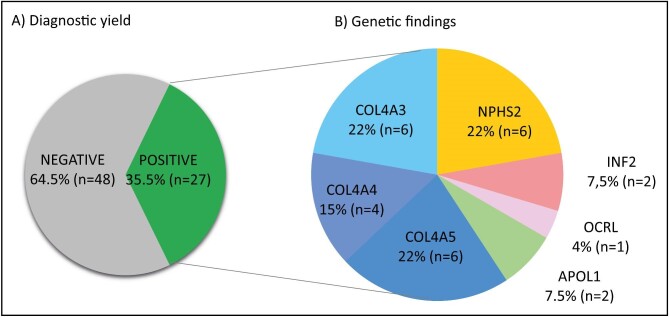
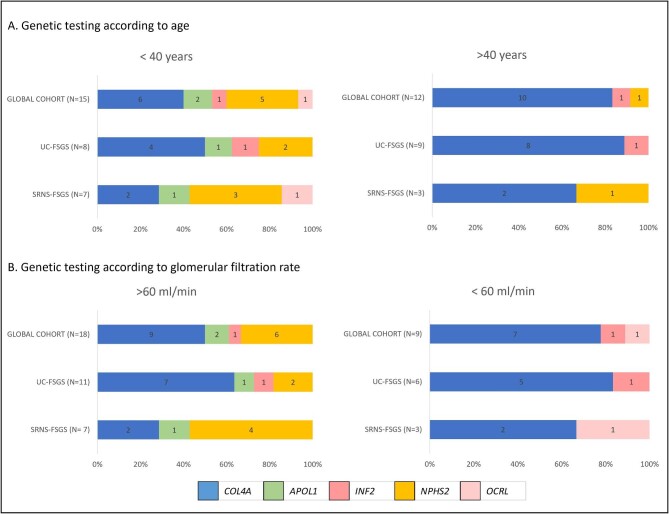
Results: Seventy-six patients met the study criteria; 24 presented with SRNS-FSGS and 52 with FSGS-UC. We detected FSGS-related disease-causing variants in 27/76 patients (35.5%). There were no differences between genetic and non-genetic causes in age, proteinuria, glomerular filtration rate, serum albumin, body mass index, hypertension, diabetes or family history. Hematuria was more prevalent among patients with genetic causes. We found 19 pathogenic variants in COL4A3-5 genes in 16 (29.3%) patients. NPHS2 mutations were identified in 6 (16.2%) patients. The remaining cases had variants affecting INF2, OCRL, ACTN4 genes or APOL1 high-risk alleles. FSGS-related genetic variants were more common in SRNS-FSGS than in FSGS-UC (41.7% vs 32.7%). Four SRNS-FSGS patients presented with NPHS2 disease-causing variants. COL4A variants were the most prevalent finding in FSGS-UC patients, with 12 patients carrying disease-causing variants in these genes.
Conclusions: FSGS-related variants were detected in a substantial number of patients with SRNS-FSGS or FSGS-UC, regardless of age of onset of disease or the patient's family history. In our experience, genetic testing should be performed in routine clinical practice for the diagnosis of this group of patients.
Keywords: FSGS; hereditary diseases; nephrotic syndrome; podocytopathy; steroid-resistant.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The authors declare that there are no conflicts of interest to disclose.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
